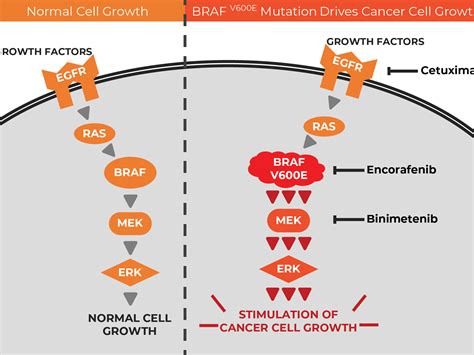
Melanoma, a particularly aggressive form of skin cancer, represents a significant global health concern. In 2022 alone, there were 331,647 new cases and 58,645 deaths reported worldwide. The development of melanoma is influenced by several factors, including exposure to sunlight and specific genetic mutations, most notably those in the BRAF gene, which can lead to the activation of the MAPK/ERK pathway. These mutations are found in approximately half of all melanomas, driving abnormal cell growth and division.
Targeted drugs are a crucial component of modern melanoma treatment. These medications are designed to specifically attack parts of melanoma cells that distinguish them from normal cells. If melanoma has spread beyond its original site, a biopsy of the cancerous tissue is typically tested to identify such gene alterations. The presence of mutations in the BRAF gene is a key factor in determining treatment strategies.
Understanding BRAF Mutations
The BRAF gene plays a critical role in regulating cell growth and division. When this gene undergoes a mutation, it can lead to uncontrolled cell proliferation, contributing to the development of cancer, including melanoma. The most common type of BRAF mutation is V600E, which accounts for about 70-80% of BRAF-mutated melanomas. Other mutations, such as V600K, occur less frequently, and rarer non-V600 BRAF mutations are found in a smaller percentage of cases.
If a melanoma tumor is found to have a faulty BRAF gene or a BRAF mutation during genetic testing, it is described as BRAF positive or BRAF mutated. This allows oncologists to consider targeted therapy as a potential treatment option. Conversely, melanomas without these specific BRAF gene changes are termed BRAF negative or BRAF wild type. It is important to note that BRAF mutations identified in cancer are typically spontaneous changes that occur during a person's lifetime and are not inherited.
Targeted Cancer Drugs for BRAF-Mutated Melanoma
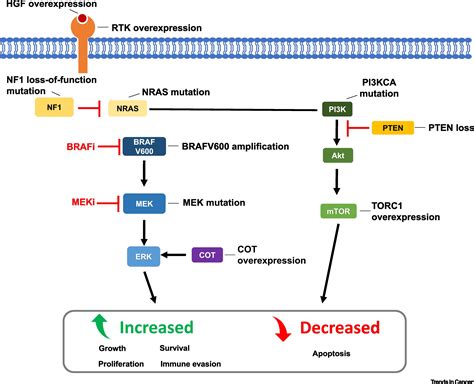
Targeted cancer drugs work by interfering with the function of abnormal molecules within cancer cells, specifically blocking the activity of mutated BRAF proteins and related proteins like MEK. The goal is to halt the mutated molecules' action, thereby slowing or stopping the growth and spread of melanoma cells without harming healthy tissue. These medications are often referred to as cancer growth blockers or inhibitors.
BRAF and MEK Inhibitors
Given that the MEK gene works in close collaboration with the BRAF gene, drugs that block MEK proteins are also effective in treating melanomas with BRAF gene alterations. The most common and effective approach involves combining a MEK inhibitor with a BRAF inhibitor. This combination therapy has demonstrated superior efficacy in shrinking tumors for longer periods compared to using either type of drug alone.
FDA-approved targeted therapy combinations for advanced melanoma include:
- Dabrafenib (a BRAF inhibitor) and Trametinib (a MEK inhibitor)
- Vemurafenib (a BRAF inhibitor) and Cobimetinib (a MEK inhibitor)
- Encorafenib (a BRAF inhibitor) and Binimetinib (a MEK inhibitor)
These targeted treatments are typically administered as tablets or capsules taken daily at home. They are used to treat melanomas that cannot be surgically removed or have spread to other parts of the body. Treatment is continued until the cancer progresses or unacceptable side effects occur. In some cases, targeted therapy, such as dabrafenib and trametinib, may be used as adjuvant treatment for up to a year after surgery if the melanoma has spread to nearby lymph nodes and all visible cancer has been removed, to reduce the risk of recurrence.
Potential Side Effects of Targeted Therapies
While targeted therapies offer significant benefits, they can also cause side effects. Common side effects associated with BRAF and MEK inhibitors may include:
- Skin thickening, rash, acne-like rash, soreness, and/or redness on the palms and soles of the feet
- Increased sensitivity to the sun, leading to a risk of severe sunburn
- Headaches and dizziness
- Fatigue and weakness
- Loss of appetite
- Hair thinning
- Muscle pain, weakness, or spasms
- Nausea and vomiting
- Diarrhea or constipation
- High temperature (fever) and chills
- High blood pressure
- Liver problems (monitored by blood tests)
- Eye problems (e.g., redness, irritation, blurred vision, pain, vision loss)
- Pain in the arms, legs, or joints
- Swelling of the hands and legs (edema)
- Trouble sleeping (insomnia)
- Low red blood cells (anemia)
- Numbness or tingling in fingers and toes
- Cough or shortness of breath (potentially indicating lung inflammation)
- Bleeding problems (mild to severe)
It is crucial for patients to report any unusual or concerning side effects to their medical team promptly. Early treatment of side effects can help manage them more effectively.
Immunotherapy for Melanoma
Immunotherapy is another powerful treatment modality for melanoma, particularly for advanced or unresectable cases. These drugs work by helping the immune system to recognize and attack cancer cells. For patients with BRAF negative melanoma, immunotherapy is typically the recommended treatment.
Checkpoint Inhibitors
A primary type of immunotherapy used for advanced and unresectable melanoma is checkpoint inhibitors. These drugs block proteins on cancer cells that prevent the immune system from attacking them, thereby unleashing the immune response against the tumor. Commonly used checkpoint inhibitors include:
- Ipilimumab (Yervoy)
- Pembrolizumab (Keytruda)
- Nivolumab (Opdivo)
Combinations of these drugs, such as nivolumab and ipilimumab, or nivolumab and relatlimab (Opdualag), are also employed. Immunotherapy is usually administered intravenously as a drip into the bloodstream.
Immunotherapy for BRAF Positive Melanoma
Interestingly, even for patients with BRAF positive melanoma, immunotherapy can be a treatment option, either instead of or in combination with targeted therapies. Clinical trials, such as the DREAMseq trial, have investigated the optimal sequencing of treatments. Results from DREAMseq indicated that patients with BRAF-mutant melanoma who initially received a combination of immunotherapy drugs (ipilimumab and nivolumab) had better overall survival at two years compared to those who started with a combination of targeted therapies (dabrafenib and trametinib). This suggests that immunotherapy can be a highly effective first-line treatment for BRAF-mutant melanoma, with targeted therapy potentially used later if the disease progresses.
However, there are scenarios where targeted therapy might be used first, such as in cases of immediately life-threatening BRAF-mutant metastatic disease, to stabilize the patient's condition before initiating immunotherapy.
Other Immunotherapy Approaches
Doctors may also utilize another form of immunotherapy called talimogene laherparepvec (T-VEC). This involves injecting a weakened, altered form of the cold sore virus directly into the melanoma. The virus is engineered to grow within cancer cells, destroy them, and stimulate an immune response against the cancer. T-VEC may be used for melanomas that cannot be removed by surgery and have spread to the lymph nodes or other nearby skin or soft tissues.
Clinical Trials and Future Directions
Research into melanoma treatment is ongoing, with a continuous effort to develop new and more effective targeted and immunotherapy drugs. Clinical trials play a vital role in evaluating these novel therapies and optimizing existing treatment strategies.
Triplet Combinations
Current research is also exploring the potential of three-drug combinations, or even four-drug combinations, to overcome treatment resistance and improve outcomes. Triplet combinations involving a BRAF inhibitor, a MEK inhibitor, and a checkpoint immunotherapy have shown promise in clinical trials for patients with immediately life-threatening BRAF-mutant metastatic melanoma, demonstrating significant improvements in progression-free survival compared to targeted therapy alone.
Adjuvant Therapy and Optimized Use of Targeted Therapy
There is ongoing discussion about optimizing the use of BRAF-targeted therapy. Some studies suggest that BRAF-targeted therapy may be most effective in patients with a lower tumor burden, potentially making it a valuable adjuvant therapy used after surgery to reduce the risk of melanoma recurrence. Clinical trials are needed to confirm this hypothesis.
Addressing Resistance and Vascular Complications
Innate and acquired resistance to BRAF-targeted therapies remains a significant challenge. Researchers are investigating potential druggable targets, such as ERK5, CD73, ALDH1A1, PLA1A, and DMKN, to address diagnostic hurdles and guide personalized therapeutic decisions. Furthermore, the off-target effects of BRAF inhibitors on endothelial cells, which can lead to vascular complications and potentially enhance metastatic potential, highlight the need for more selective therapies or strategies to mitigate these side effects.
MOA Animation: Melanoma BRAF Inhibition
The ongoing synergy between advancing research, targeted interventions, strategic treatment combinations, and cost-effectiveness evaluations offers a promising pathway to significantly improve patient outcomes in the persistent battle against melanoma.