Are you bothered by rough or waxy spots on your face or body? You may be dealing with seborrheic keratoses-harmless but often annoying skin growths that many people choose to remove for a smoother, more refreshed appearance.
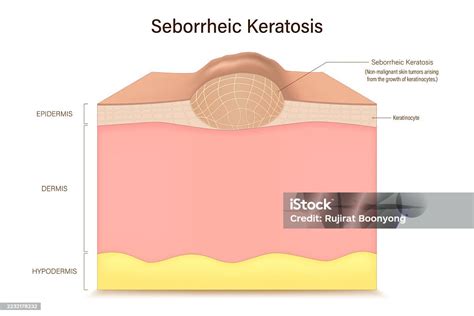
A seborrheic keratosis (seb-o-REE-ik ker-uh-TOE-sis) is a common benign skin growth, similar to a mole. Most people will have at least one in their lifetime. They tend to appear in mid-adulthood and their frequency increases with age. They are harmless and don’t require treatment, but you can have them removed if they bother you. Skin growths like seborrheic keratoses are sometimes also called epidermal tumors. That doesn’t mean they’re cancer, though. Technically, moles and warts are also epidermal tumors. That just means they are clusters of extra cells on the epidermis, the outer layer of the skin. They aren’t considered a risk factor for skin cancer.
What Seborrheic Keratosis Looks Like
Seborrheic keratoses are roundish or oval-shaped patches on the skin with a “stuck on” appearance. They are sometimes described as waxy or scaly. They are raised above the skin, and even when they are flat, you can feel them with your finger. They are usually brown, but can also be black or tan, and less often, pink, yellow, or white. They often appear in numbers.
Seborrheic keratoses are characterized by keratin on the surface-the same fibrous protein that fingernails, hooves, and horns are made of. This causes the textural details that often distinguish the growths. Sometimes it looks like small bubbles or cysts within the growth. Sometimes it looks scabby or wart-like. Sometimes it looks like the ridges and fissures in a brain.
Who Gets Seborrheic Keratosis?
Anyone can get one, but most commonly:
- People who are 50 and older. They usually begin to appear in middle age, and rarely in younger people. About 30% of people have at least one by the age of 40, and about 75% by the age of 70.
- People with a family history of it. About half of all cases of multiple seborrheic keratoses occur in families, suggesting that the tendency to develop many of them may be inherited.
- Lighter-skinned people. Classic seborrheic keratosis as described here appears less frequently in darker-skinned people.
“Seborrheic keratoses are a very common skin finding, and most people will develop at least a few throughout their lifetime. Doctors and researchers do not know the exact cause of seborrheic keratoses. No, seborrheic keratoses are not contagious. “Seborrheic keratoses cannot be transferred from one person to the next. While SKs are benign and do not require medical attention. Seborrheic keratoses are typically painless. Seborrheic keratoses typically do not require treatment.
Diagnosis of Seborrheic Keratosis
Your doctor can usually tell whether you have a seborrheic keratosis by looking at the affected skin. If there is a question about the diagnosis, your doctor might recommend removing the growth so that it can be examined under a microscope.
Treatment Options for Seborrheic Keratosis
A seborrheic keratosis typically doesn't go away on its own, but treatment isn't always needed. Your doctor will work with you to determine the most appropriate treatment option based on the size, location, and number of your SKs.
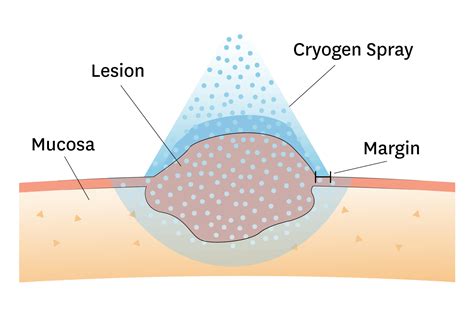
Cryotherapy (Freezing)
Dermatologists often opt for the liquid nitrogen freezing technique, known as cryotherapy, to treat seborrheic keratosis. This method is popular due to its effectiveness and ease of use. Choosing this treatment option means you'll experience a simple and effective process. The dermatologist will start by cleaning the surface of the seborrheic keratosis, then gently apply liquid nitrogen. You will feel a brief cold sensation when the nitrogen touches your skin, but it usually subsides quickly. This procedure is very fast, often taking just a few seconds for each growth, making cryotherapy a great option for those with multiple keratoses.
According to the American Academy of Dermatology, cryotherapy boasts an impressive 90% success rate in effectively treating small seborrheic keratosis. Patients undergoing cryotherapy might experience mild discomfort during treatment-imagine a brief sting followed by numbness-but any sensations should dissipate immediately. Choosing cryotherapy for seborrheic keratosis treatment combines cutting-edge technology with rapid results. Cryotherapy is a popular choice because it’s both quick and cost-effective. In just a few minutes, a healthcare professional can apply nitrogen to freeze off the growths, leading to swift results and minimal discomfort. However, this method does come with a cautionary note. It may take more than one application to completely remove an SK.
Cryosurgery is a highly effective treatment for a broad range of benign skin problems. With appropriate instruction and supervised experience, family physicians can master the technique quickly. Cryosurgery is best suited for use in patients with light skin and for treatment of lesions in most non-hair-bearing areas of the body. Spray methods include the timed spot freeze technique, the rotary or spiral pattern, and the paintbrush method. Benign skin lesions that are suitable for freezing include actinic keratosis, solar lentigo, seborrheic keratosis, viral wart, molluscum contagiosum, and dermatofibroma. Cryosurgery requires little time and fits easily into the physician’s office schedule. Advantages of this treatment include a short preparation time, low risk of infection, and minimal wound care. In addition, cryosurgery requires no expensive supplies or injectable anesthesia, and the patient does not have to return for suture removal. Potential side effects include bleeding, blister formation, headache, hair loss, and hypopigmentation, but rarely scarring. Skin lesions often can be treated in a single session, although some require several treatments. Liquid nitrogen, which boils at −196°C (−320.8°F), is the most effective cryogen for clinical use. It is particularly useful in the treatment of malignant lesions. Temperatures of −25°C to −50°C (−13°F to −58°F) can be achieved within 30 seconds if a sufficient amount of liquid nitrogen is applied by spray or probe. Generally, destruction of benign lesions requires temperatures of −20°C to −30°C (−4°F to −22°F). Irreversible damage in treated tissue occurs because of intracellular ice formation. The degree of damage depends on the rate of cooling and the minimum temperature achieved. Slow thaw times and repeat freeze-thaw cycles produce more tissue injury than a single freeze and thaw. Usually, several minutes are allowed between repeat freeze-thaw cycles. Mild freezing leads to dermoepidermal separation, which is useful in treating benign epidermal lesions. The more sensitive cells in the epidermis are destroyed while the dermis is left intact. The dose of liquid nitrogen and the choice of delivery method depend on the size, tissue type, and depth of the lesion. The area of the body on which the lesion is located and the required depth of freeze also should be considered.
The timed spot freeze technique achieves temperatures that are adequate for tissue destruction in an ice field up to 2 cm in diameter. The best approach for lesions larger than 2 cm (including an adequate margin) is to use overlapping treatment fields. Variations on the open spray technique include the rotary or spiral pattern and the paintbrush method. These techniques can be useful for treating larger benign lesions. While the open spray technique can be used for the most easily accessible lesions, a cryoprobe attached to the liquid nitrogen spray gun can provide added versatility, depending on the site and type of the lesion. Various sizes and types of cryoprobes are available. The cryoprobe is applied directly to the lesions. Cryoprobes frequently are used in the treatment of smaller facial lesions (e.g., on the eyelids), where scatter of liquid nitrogen is undesirable.
Seborrheic keratosis, the most common benign neoplasm, is best treated with cryosurgery or shave excision/curettage. In treating seborrheic keratosis, the physician should consider the potential for hair loss in treated areas when choosing a therapeutic modality. The other major side effect of cryosurgery for this lesion is hypopigmentation. Warts that are resistant to over-the-counter topical agents commonly are treated with cryosurgery. However, response is variable and often depends on the size of the wart and the degree of hyperkeratosis. To avoid hypopigmentation, small flat warts may be treated with a light spray technique. Digital warts respond favorably to the timed spot freeze spray technique. Deep plantar or palmar warts present challenges, because pain may limit the patient’s tolerance of freezing. Molluscum contagiosum, a common dermatologic problem in younger persons, is caused by a poxvirus. Open spray or cryoprobe techniques may be used to improve the cosmetic appearance of dermatofibromas. A single 20- to 30-second freeze-thaw cycle is advised, and a 1- to 2-mm margin should be obtained. Retreatment in eight weeks may be necessary.
Potential side effects include bleeding, blister formation, headache, hair loss, and hypopigmentation, but rarely scarring. Hypopigmentation is common, especially with longer freeze times, but is less noticeable in light-skinned patients and improves within several months. Hypopigmentation is caused by the greater sensitivity of melanocytes to freezing, a situation that can be used to advantage in the treatment of dermatofibromas, which frequently have some mild overlying hyperpigmentation.
Curettage (Scraping)
This procedure involves using a specialized instrument called a curette, which resembles a small scooping tool. What makes curettage particularly beneficial is its precision. Because it allows dermatologists to visualize the affected area closely while removing the growths, they can ensure that all unwanted tissue is cleaned away thoroughly. This meticulous detail contributes significantly to minimized scarring and aids in achieving smooth skin post-treatment.
During curettage, your dermatologist scrapes away the seborrheic keratosis with a surgical instrument. Sometimes shaving or scraping is used along with cryosurgery to treat thinner or flat growths. Immediate aftercare is typically straightforward following curettage. Patients may notice some redness or slight crusting at the treated site, similar to having scraped skin-this is completely normal and generally fades within days. It’s essential to keep the area clean and avoid excessive sun exposure while it heals. Patients returning for follow-up visits will often see rapid improvements as their skin begins to heal. Curettage is effective and provides tangible results with minimal discomfort, making it a popular choice for many seeking treatment for seborrheic keratosis.
On the other hand, curettage offers another layer of effectiveness. The small instrument used in this procedure allows for precise scraping of the seborrheic keratosis. Many find satisfaction in knowing that this thorough approach helps ensure complete removal of the growth. However, patients should be aware that there may be a trade-off; there is a very small possibility of scarring post-procedure.
Scalpel Technique
At our practice, we offer expert removal of seborrheic keratoses, using a precise scalpel technique. After local anesthesia is injected, the keratosis is removed with a scalpel. This meticulous method is especially well-suited for the face. Healing typically occurs within a week, and there's very little risk of scarring.
At our Upper East Side dermatology office in NYC, Dr. Debra Jaliman brings over 25 years of experience in treating these growths with a gentle, precise scalpel technique that typically leaves no marks or scarring. The procedure is quick, performed right in our office with just a bit of local numbing, and most patients heal with ease.
Electrosurgery (Burning)
Electrosurgery is a common and effective treatment for seborrheic keratosis removal. At Dr. Debra Jaliman’s Upper East Side dermatology office in New York City, this in-office procedure uses a focused electrical current to safely burn off the growth. For many patients, electrosurgery is combined with curettage (a gentle scraping technique) to fully remove the seborrheic keratosis and reduce the chance of recurrence. The procedure is quick and performed under local anesthesia. Electrosurgery is ideal for treating flat or slightly raised seborrheic keratoses and typically results in excellent cosmetic outcomes.
First, your doctor will numb the area and then destroy the growth with electrocautery. Electrosurgery treatments typically cause mild redness for several days, followed by scab formation.
Laser Treatment
Laser treatment is a precise, non-invasive option for removing seborrheic keratoses with minimal discomfort and excellent cosmetic results. The laser works by delivering focused energy to the pigment and cells in the seborrheic keratosis, breaking them down so the lesion gradually fades or sloughs off. Laser removal is quick, often requiring no anesthesia or only a topical numbing cream. There’s little to no downtime, and most patients can return to normal activities immediately.

Aftercare and Recovery
Your recovery time depends on the treatment method chosen by your doctor. A scab will develop and naturally fall off within 2-4 weeks. Your doctor will provide specific aftercare instructions for any treatment method. “Recovery from SK removal is typically straightforward and well-tolerated by most patients, with healing progress visible week by week.
Choosing a Dermatologist
Choosing a skilled and experienced dermatologist like Dr. Debra Jaliman is essential for effectively treating seborrheic keratosis or any skin issue. It's important to seek a professional who comprehends the details of your condition and tailors their care to your specific requirements.
- Experience: Consider the dermatologist's years of experience in treating seborrheic keratosis.
- Reviews: Browse online feedback or seek suggestions from friends.
- Trust your gut feelings: If something seems off during your initial visit or if their way of communicating doesn't sit well with you, feel free to look for another professional. Your health and comfort are the top priority; it's essential to find a dermatologist who connects with you personally to help you maintain your confidence during the treatment.
By thoughtfully evaluating these factors before choosing your dermatologist, you set yourself up for effective care that addresses your unique skin issues. Seeking a specialist for seborrheic keratosis treatment is a significant step towards healthier skin.
Schedule your consultation with Dr. Debra Jaliman today.
Important Considerations
No, it is noncancerous. Minimal discomfort. Local anesthesia is used. There is usually no scar if done by a skilled dermatologist.
Talk with your doctors about the risks and benefits of each method. Some methods can cause permanent or temporary skin discoloration and scarring. After treatment, you might develop a new seborrheic dermatosis elsewhere on your body.
Seborrheic keratoses do not develop into skin cancer. It’s important to monitor your skin for unexpected changes such as rapid growth, unexplained bleeding, color changes, persistent discomfort, or irregular borders. A practical approach is to document your existing growths and note any changes over time. Our experienced staff can provide personalized advice and treatment options to address your specific needs.
Common complications and side effects of cryosurgery are listed in Table 3. Skin discomfort, generally a burning sensation, occurs with cryosurgery, but intensity is variable. The most sensitive areas are the fingertips, ears, and temples. Freezing of lesions on the forehead or temple may produce headaches.
Cryo Surgery Procedure (Freezing)
tags: #freezing #seborrheic #keratosis