A patient, a 50-year-old male, experienced a breakout of what he described as upper body hives and flushing following a knee replacement surgery. This reaction began concurrently with a new medication regimen that included celecoxib, aspirin (81 mg), metoclopramide, famotidine, bisacodyl, and an additional 81 mg of aspirin. He was prescribed a 30-day supply of these medications. The patient underwent two courses of oral steroids, and he discontinued celecoxib approximately 20 days into the course due to suspicion that it might be causing the reaction. He continued taking aspirin, believing it could help reduce the risk of blood clots. Despite ceasing celecoxib, the rash persisted until around day 30 of his medication course. Previously, he had tolerated ibuprofen without issue.
Potential Causes of Post-Surgical Rashes
Post-surgical rashes can manifest for various reasons, often related to the surgical procedure itself, the materials used, or medications administered. Understanding the potential causes is crucial for effective diagnosis and management.
Contact Dermatitis
Post-surgical contact dermatitis is a localized rash that typically results from direct contact with a substance. Given that any surgery involves exposure to numerous materials and medications, individuals with allergies or skin sensitivities are at a higher risk of developing this type of rash. The National Eczema Association categorizes contact dermatitis into two main forms:
- Irritant Contact Dermatitis: This is the more common form, accounting for about 80% of cases. It involves skin irritation or inflammation caused by direct contact with a chemical, biological, or physical agent.
- Allergic Contact Dermatitis: This form, making up the remaining percentage, occurs when the immune system overreacts to an allergen, leading to skin irritation and inflammation.
Both types of contact dermatitis are usually confined to the areas of skin that have come into contact with the offending substance or irritant. The American Academy of Allergy, Asthma and Immunology notes that up to 20% of the population experiences contact dermatitis. While the exact incidence of post-surgical rashes is not precisely known, individuals with a prior history of contact dermatitis may be more susceptible to similar reactions after surgery.

Medication Reactions
Medications, both topical and systemic, are common culprits for post-surgical rashes. Topical medications, such as antibiotic creams applied directly to wounds, can irritate the skin or trigger an allergic response. Systemic medications, including pain relievers and antibiotics commonly administered during or after surgery, can also lead to generalized or localized rashes.
Specific Medication Considerations
In the case presented, the patient was taking a combination of medications, including celecoxib and aspirin, which are nonsteroidal anti-inflammatory drugs (NSAIDs). NSAID hypersensitivity reactions are often mediated by the pharmacological inhibition of the COX-1 enzyme rather than an immunologic response. While the exact cause of the patient's rash was not immediately clear, aspirin was considered a primary suspect. However, the patient's urticaria persisted even after discontinuing celecoxib, suggesting a potential reaction to other medications or a more complex underlying cause.
It's important to note that while selective COX-2 inhibitors like celecoxib are generally better tolerated by patients with a history of COX-1 hypersensitivity, reactions have been reported. The low dose of aspirin (81 mg daily) might be considered too low to elicit a significant reaction in some individuals, but this is not a definitive rule.
Autonomic Denervation Dermatitis (ADD)
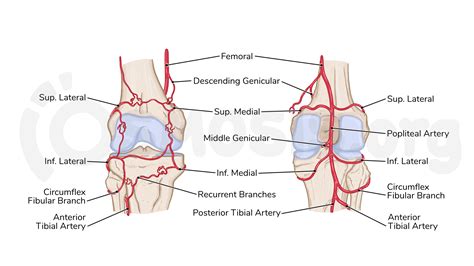
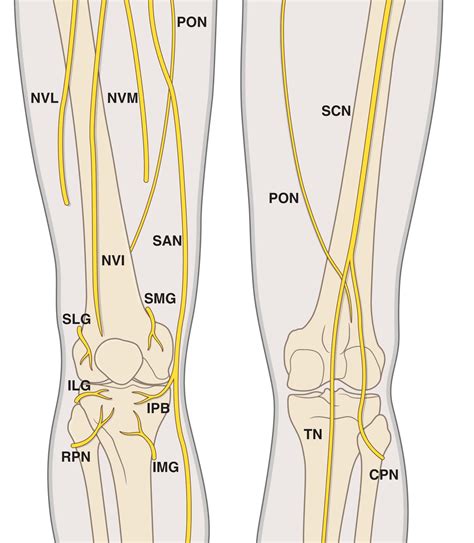
Autonomic Denervation Dermatitis (ADD) is a less common, localized eczematous eruption that can occur around a surgical incision site, particularly after total knee replacement (TKR) surgery. It is thought to result from denervation injury due to the transection of dermal nerve fibers during surgery and subsequent autonomic disruption. ADD is often associated with cutaneous sensory loss in the distribution of the infrapatellar branch of the saphenous nerve following TKR through an anterior midline incision. Diagnosis is typically clinical, and patch testing is often negative and not routinely required. ADD generally responds well to topical emollients and corticosteroids.
Surgical Supplies
Materials used during surgery can also contribute to a rash. This includes non-hypoallergenic supplies such as surgical glue or adhesives used for wound closure, antiseptic prep solutions, surgical dressings like bandages and tape, and even rubber products like blood pressure cuffs. These items can cause irritant contact dermatitis or trigger an allergic reaction.
Symptoms of Post-Surgical Rashes
The symptoms of post-surgical rashes can vary depending on the cause but commonly include:
- Itchiness or burning sensation
- Redness or discoloration of the skin
- Mild swelling
- Skin blisters that may drain fluid, especially if scratched
- Thickening or scaling of the skin
- Bumps on the skin
In some cases, additional symptoms may accompany the rash, such as fever, oozing or weeping from the rash, or pain. It is crucial to differentiate a rash from a surgical site infection, which may present with similar signs like redness, heat, or discharge.
Diagnosis of Post-Surgical Rashes
Diagnosing the cause of a post-surgical rash involves a comprehensive approach:
- Health History and Physical Exam: A doctor will review the patient's medical history, including medications, allergies, and previous skin conditions. A physical examination of the rash will assess its characteristics, such as size, shape, color, and severity.
- Drug Provocation Testing: For suspected drug allergies, particularly NSAIDs, controlled drug provocation testing may be necessary to identify the offending agent. This is often the only way to definitively rule in or rule out a specific drug.
- Patch Testing: This test is used to identify allergens in cases of suspected allergic contact dermatitis.
- Skin Biopsy: In some complex or persistent cases, a skin biopsy may be performed to aid in diagnosis.

Treatment Options for Post-Surgical Rashes
Treatment for post-surgical rashes depends on the underlying cause:
General Management
If a rash is diagnosed as contact dermatitis, the primary treatment involves avoiding the identified irritant or allergen. For both irritant and allergic contact dermatitis, several home and over-the-counter (OTC) treatments can provide relief:
- OTC antibiotic creams (e.g., Polysporin)
- OTC cortisone creams
- Cold compresses
- Calamine lotion
- Colloidal oatmeal baths
Note: Many healthcare professionals advise against the routine use of OTC Neosporin due to the potential for allergic contact reactions.
Prescription Medications
A doctor may prescribe medications to manage more severe or persistent rashes:
- Prescription antihistamines to alleviate itching
- Prescription cortisone creams for inflammation
- Antibiotics if the rash is due to a bacterial infection
- Steroid pills for severe rashes
- Prescription anti-inflammatory medications
- Replacement medication if the rash is a confirmed drug allergy
NSAID Management and Challenges
For patients experiencing NSAID-related rashes, a stepwise approach to pain management is often considered. Given that the patient tolerated ibuprofen previously, a challenge with ibuprofen might be considered, especially since his urticaria persisted despite discontinuing celecoxib and potentially reacting to aspirin. However, caution is advised due to the possibility of cross-reactivity among NSAIDs, particularly those that inhibit COX-1. While selective COX-2 inhibitors are generally safer, individual reactions can still occur.
Controlled drug provocation challenges are the gold standard for diagnosing NSAID hypersensitivity. In cases of NSAID-induced urticaria and/or angioedema (NIUA), desensitization can be an option, although it is not recommended for NSAID-exacerbated cutaneous disease (NECD).
Pharmacology - Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
When to Seek Emergency Care
A rash can sometimes be an early sign of a life-threatening allergic reaction known as anaphylaxis. The American Academy of Dermatology Association (AADA) recommends seeking emergency care immediately if any of the following symptoms are present:
- Shortness of breath or difficulty breathing
- Swelling in the eyes or lips
- A rash that appears quickly, spreads rapidly, and covers a large portion of the body
- Fever accompanying the rash
- A rash that is painful to the touch
- Blisters associated with the rash
- Signs of infection, such as a rash that appears infected
It is essential to contact your doctor immediately if your wound or the surrounding area becomes red, discolored, hot, or itchy, or if there is any discharge of green, yellow, or cloudy fluid, as these can indicate an infection requiring prompt treatment.
tags: #itchy #rash #after #knee #replacement