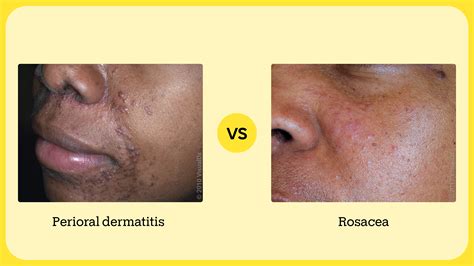
Perioral dermatitis, also known as periorificial dermatitis, is a common inflammatory skin condition characterized by a red rash that typically encircles the mouth. The affected skin can appear scaly, dry, and flaky, often accompanied by swollen, inflamed bumps called papules. This condition can be easily mistaken for acne due to its similar appearance, with some individuals reporting itching or burning sensations. In some cases, the rash may extend to the nose, eyes, and, very rarely, the genitals.
The name "perioral" literally means "around the mouth" (peri - around, oral - mouth), while "periorificial" signifies "around an opening," both referring to the same condition's characteristic location.
Types of Perioral Dermatitis
There are two main presentations of perioral dermatitis:
- Typical Perioral Dermatitis: This is the most common form, presenting with red papules and a rash around the mouth.
- Granulomatous Perioral Dermatitis: This is considered an irregular or more severe variant. Instead of red bumps, individuals with this type may develop yellowish bumps. Children are more frequently affected by this form than adults.
Common Locations and Spread
The rash of perioral dermatitis is most recognizable by its presence around the mouth. However, it can also affect the eyelids, the area around the eyes, and the nose. Less commonly, it may appear on the genitals, ears, neck, scalp, trunk, and extremities.
Potential for Recurrence and Rosacea
Perioral dermatitis can recur even after successful treatment. In many instances, these recurring cases can develop into rosacea, another skin condition characterized by red papules, often affecting the central face, including the nose.
Risk Factors and Demographics
While perioral dermatitis can affect individuals of all ages, sexes, and ethnicities, certain groups are at higher risk:
- Women between the ages of 25 and 45 are most commonly affected.
- Individuals who use topical steroids, face creams, and other cosmetic products are also at increased risk.
- Children and men can also develop perioral dermatitis.
It is important to note that no type of dermatitis is contagious and cannot be spread from person to person.
Suspected Causes and Contributing Factors
The exact cause of perioral dermatitis remains unknown, and several theories exist. While some suspect a link to Candida albicans (a type of yeast), the most commonly implicated factor is the overuse of topical steroids.
Other potential triggers and contributing factors include:
- Topical steroids: Applied intentionally or accidentally to the face.
- Nasal steroids, steroid inhalers, and oral steroids.
- Cosmetic products: Including creams, make-ups, and sunscreens.
- Fluorinated toothpaste.
- Failure to wash the face adequately.
- Hormonal changes or the use of oral contraceptives (interestingly, oral contraceptives have been associated with improvement in some cases).
- Chewing gum and dental materials.
- Facemask use (especially in recent years).
- Improper use of activated oxygen in CPAP machines.
Skin irritants that cause the breakdown of the top layer of the skin may also contribute to the development of perioral dermatitis.

Symptoms of Perioral Dermatitis
The symptoms of perioral dermatitis can vary but commonly include:
- A burning or sensitive feeling around the mouth, particularly in the creases between the nose and mouth.
- Small, red, inflamed bumps (papules) around the mouth, which may sometimes be filled with fluid or pus. These can resemble acne.
- A similar rash may appear around the eyes, nose, or forehead.
- Scaling, dryness, and flaking of the skin.
It is important to note that the vermilion borders of the lips are typically spared in perioral dermatitis.
Diagnosis
Perioral dermatitis is primarily diagnosed clinically based on its characteristic appearance and location. A healthcare provider will examine the skin. In atypical cases or if the condition does not respond to initial treatment, further tests such as a skin biopsy, bacterial culture, or a potassium hydroxide (KOH) prep (to rule out fungal infection) may be performed.
Differential Diagnosis
Several other skin conditions can mimic perioral dermatitis, making differential diagnosis important:
- Rosacea: Characterized by inflammatory papules, pustules, and facial redness, often with flushing and visible blood vessels. Some experts consider perioral dermatitis a variant of rosacea.
- Acne Vulgaris: Distinguished by the presence of comedones (blackheads and whiteheads) in addition to inflammatory lesions.
- Sarcoidosis: Can present with papules on the face but is typically more widespread and may involve systemic symptoms.
- Seborrheic Dermatitis: Presents as erythematous patches with greasy scales, commonly affecting eyebrows, glabella, and nasolabial folds.
- Allergic Contact Dermatitis: May present with scaling and redness; patch testing can help identify triggers.
- Irritant Cheilitis: Affects the vermilion border of the lips.
- Demodex Folliculitis: Characterized by scattered papules and pustules, with Demodex mites being implicated.
- Tinea Faciei: A fungal infection presenting as erythematous, scaling patches or annular plaques.
- Cutaneous Adnexal Neoplasms: Such as syringomas, which appear as flesh-colored to erythematous papules.
Treatment Strategies
Effective treatment of perioral dermatitis often requires a multi-faceted approach and can take several weeks to months. Key strategies include:
1. Discontinuation of Triggering Agents
The cornerstone of treatment is to immediately stop using any products that may be contributing to the condition. This includes:
- Topical steroids: This is crucial, as steroids can initially seem to help but ultimately worsen the condition and lead to dependency. Abrupt cessation can cause a rebound flare, so a gradual taper under medical supervision may be necessary.
- Cosmetics, heavy creams, and sunscreens.
- Fluorinated toothpaste.
2. Skincare Regimen
Adopt a gentle skincare routine:
- Wash the face with warm water only initially.
- Once the rash has cleared, use a non-soap bar or a gentle, fragrance-free, exfoliant-free liquid cleanser and moisturizer.
- Adhere to a minimal therapy approach, avoiding potential skin irritants.
3. Topical Medications
Several topical medications may be prescribed by a healthcare provider:
- Metronidazole
- Erythromycin
- Benzoyl peroxide
- Tacrolimus
- Clindamycin
- Pimecrolimus
- Sodium sulfacetamide with sulfur
4. Oral Antibiotics
For more severe cases, oral antibiotics are often necessary. These are typically used for 6 to 12 weeks, sometimes longer, with a gradual tapering course:
- Tetracycline (250-500 mg twice daily)
- Doxycycline (100 mg twice daily or once daily)
- Minocycline (100 mg twice daily or once daily)
- Erythromycin (250-500 mg daily) may be used when tetracyclines are contraindicated (e.g., in children under 8, nursing mothers, or pregnant females).
The goal of oral antibiotic therapy is to achieve rapid improvement, with topical therapies used concurrently. Peak efficacy of topical treatments may not be seen for up to 3 months.
5. Other Treatments
For the granulomatous variant, treatments like 1.5% topical ruxolitinib cream have shown promising results.
Topical steroids || Topical steroids Dermatology || Topical steroids Pharmacology #dermatology
Prognosis and Complications
Perioral dermatitis can be a chronic, relapsing condition, and treatment may require several months. While many patients recover well with appropriate management, potential complications include:
- Emotional distress due to the chronic nature and visible lesions.
- Poor quality of life stemming from the disfiguring nature of the rash.
- Scarring, particularly with the lupoid variant.
Even after successful treatment, the rash may return in some individuals.
Prevention and Patient Education
Prevention and patient education are vital for managing perioral dermatitis:
- Understand triggers: Be aware of potential triggers, especially the harmful effects of topical corticosteroids, including over-the-counter products.
- Discontinue offending agents: Strictly avoid all topical steroids and other potential irritants like harsh cosmetics and fluorinated toothpaste.
- Realistic expectations: Understand that treatment can take time, and a temporary worsening (rebound flare) may occur after stopping steroids.
- Adherence to treatment: Follow the prescribed regimen consistently and complete the full course of treatment, even after the rash appears to be gone.
- Open communication: Maintain open communication with your healthcare provider about any concerns or side effects.
tags: #perioral #dermatitis #flaking