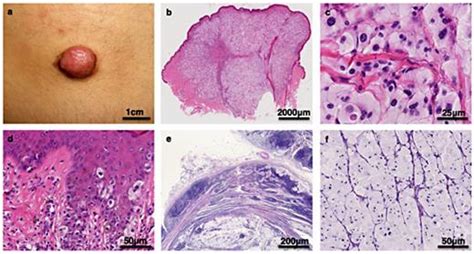
Balloon cell melanoma (BCM) represents a rare and diagnostically challenging histological variant of malignant melanoma, accounting for less than 1% of all such cases. This entity presents a unique morphology characterized by tumor cells with abundant clear or eosinophilic granular cytoplasm, leading to a ballooning appearance. The tumor cells may contain Periodic Acid-Schiff (PAS)-positive, diastase-resistant granules, which are composed of ribonucleoprotein. These characteristic features are thought to result from either abnormal melanosome metabolism or melanosome degeneration.
Introduction
Malignant melanoma poses a significant global health challenge due to its rising incidence and prevalence, underscoring the critical importance of prevention. The histological diagnosis plays a fundamental role in the correct classification of the neoplasm, guiding therapeutic decisions. However, melanoma diagnosis can be complex, frequently requiring integration with immunohistochemical and molecular data. Melanoma can also arise in non-cutaneous sites, including mucous membranes such as the oral cavity, vagina, and intestine. In this context, balloon cell melanoma (BCM) emerges as a rare and unusual entity that can manifest as either a primary lesion or a metastasis.
Historically, various explanations have been proposed for the morphological changes observed in BCM. Current understanding, supported by electron microscopy studies, suggests that an overproduction of swollen and defective melanosomes is the underlying cause of this specific morphotype.
Materials and Methods
This study involved a retrospective analysis of cases from the Odontomatostologic Clinic's laboratory archive, spanning from January 1, 2008, to December 31, 2021. Cases were identified by searching for the term "Balloon Cell" within the electronic database, specifically targeting malignant melanoma diagnoses.
Sections stained with Hematoxylin/Eosin (H&E) and corresponding tissue blocks were retrieved and re-evaluated by two experienced skin pathologists. Disagreements were resolved through consultation with a third dermatopathologist. Clinical information was obtained from referring dermatologists and plastic surgeons, with direct contact to patients or their families if necessary.
Additionally, a systematic literature review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Databases such as PubMed, Web of Science (WoS), and Scopus were searched for articles published between 1970 and 2021 using the terms "balloon cell melanoma" and "melanoma with balloon cell," combined with "dermatopathology" and "skin." Only English-language articles were included. The final search was performed on December 31, 2021. Eligible articles were assessed based on the Oxford Centre for Evidence-Based Medicine 2011 guidelines. Review articles, meta-analyses, observational studies, case reports, survey snapshot studies, letters to the editor, and comments were all considered. References from included literature were manually reviewed to identify additional relevant articles. Two investigators independently extracted data according to the inclusion criteria, with disagreements resolved through discussion.
Results
Clinicopathological Characteristics of Local Cases
Four cases of balloon cell melanoma were identified from the electronic database. The clinical-pathological characteristics of these cases are detailed in Table 1 (not provided in the original text, but implied). Two male patients (50.0%) and two female patients (50.0%) were included, with BCM occurring in four different body locations. In three of the four cases (75.0%), the initial clinical suspicion was malignant melanoma.
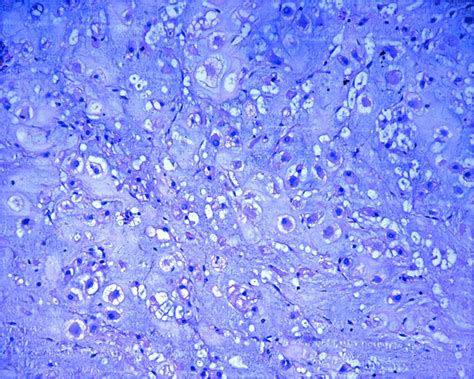
Microscopically, all four lesions exhibited characteristic features, with more than 50% of the melanocytes displaying a "balloon-shaped" morphology. These cells were distinguished by abundant, finely vacuolized cytoplasm and hyperchromatic nuclei, typically located peripherally but not pyknotic. Mitotic activity was rare, and melanin content was reduced and dispersed irregularly within the cells and in numerous melanophages. Architecturally, the cells were organized in large, pale masses that replaced the dermis and thinned the epidermis. These solid sheets of ballooniform melanocytes were delineated by thin collagenous septa. No clear signs of activity at the dermo-epidermal junction or pagetoid spread were observed. In one case, a component of "spindle cell" melanoma was also noted.
Immunohistochemical Findings
Immunohistochemical analysis of the four cases revealed consistent expression of S-100 protein and Melan-A. Additionally, positivity for HMB-45 and SOX-10 was observed in all cases.
Literature Review Findings
The systematic literature search initially identified 137 records, with 33 duplicates. After screening and applying eligibility criteria, 70 publications were included in the final analysis. The majority of these publications were case reports (n=51), followed by reviews (n=10), case series (n=6), and editorials (n=3). All included studies were rated as evidence level 4 or 5 according to the Oxford Centre for Evidence-Based Medicine 2011 guidelines. In total, 115 patients with primary and/or metastatic balloon cell melanoma were described in the literature.
Distribution of Primary Lesions and Metastases
Of the 115 patients, primary lesions were most frequently reported on the back (36 patients, 31.3%), followed by the extremities (20 patients, 17.4%-17 in upper limbs, 3 in lower limbs). Other primary sites included the head/neck (11 patients, 9.6%), choroid or ciliary body (9 patients, 7.8%), and conjunctiva (2 patients, 1.7%). Metastases were present at the time of observation in 15 patients (13.0%), and the primary site was unknown in 9 cases (7.8%). Less common primary sites included the orbit (2 cases, 1.7%), chest (2 cases, 1.7%), anal canal (6.9%), and urethra (1 case).
The mean age of patients was 54 years, with lesion dimensions ranging from 0.3 to 5 cm in maximum diameter. Immunohistochemical findings in the literature review indicated near 90% positivity for S-100 protein and HMB-45. Neuron-Specific Enolase (NSE) was positive in 7% of cases, and carcinoembryonic antigen (CEA) was expressed in 23.5% of lesions.
In most cases, the clinical suspicion was an atypical pigmented lesion suggestive of malignant melanoma. Amelanotic lesions were noted in a smaller proportion of cases.
Discussion
Malignant melanoma remains a prevalent and rapidly increasing malignancy worldwide. Histopathological diagnosis is considered the gold standard for guiding subsequent diagnostic and therapeutic steps. Accurate morphological and immunohistochemical recognition is crucial for improving patient outcomes, with five-year survival rates varying significantly based on disease stage.
Among the diverse histological patterns of melanoma, unusual and rare forms, such as balloon cell melanoma (BCM), are of significant importance to avoid misdiagnosis. BCM is a very rare variant, defined by the presence of at least 50% of melanocytes exhibiting a ballooniform histological appearance. Since the first report by Gardner in 1970, descriptions of BCM have increased, with approximately 115 patients reported in the literature up to the present study.
The analysis of included studies reveals that the most common primary localizations for BCM are the back, extremities, choroid, and head/neck region, with rare cases originating from the conjunctiva. This distribution pattern, with a predominance of lesions on the back, was also observed in the four new cases presented in this paper (two on the back, one on the left leg, and one on the right flank).
Similar to findings in the literature, the presented cases lacked distinctive clinical characteristics, with the general clinical suspicion being malignant melanoma. Recent research has explored potential dermoscopic criteria suggestive of BCM, such as yellowish structureless areas, white lines, and irregular hairpin-shaped or curved vessels.
Regarding prognosis, the available data suggest that BCM does not appear to have a substantially different prognosis compared to conventional melanoma. The outcome remains largely dependent on the Breslow thickness of the tumor, indicating that the degree and depth of balloon cell changes do not independently influence prognosis.
Differential Diagnosis
A critical aspect for dermatopathologists is the differential diagnosis of BCM with benign and malignant lesions exhibiting ballooniform cells, such as balloon cell nevi, or other clear cell neoplasms. Distinguishing between a balloon cell nevus and BCM can be challenging due to their similar presentation. Extensive examination of the sample may be necessary to identify areas of conventional malignant melanoma, which can aid in diagnosis. In cases with less atypical melanocytes and without significant cytological features, a diagnosis of balloon cell nevus may be considered. Consideration should also be given to Spitz balloon cell nevi, particularly in individuals under 20 years of age, where specific histological features can guide diagnosis.
BCM can also be confused with non-melanocytic entities. Classic differential diagnoses include renal cell carcinoma, clear-cell sarcoma (malignant melanoma of soft parts), xanthoma, hibernoma, and clear-cell carcinomas of various organs. While some authors have proposed a distinction between clear-cell melanoma and BCM, it is advisable to avoid the term "clear-cell melanoma" to prevent confusion with clear-cell sarcoma. Other entities to consider include clear-cell syringoma, granular cell tumor, malignant eccrine acrospiroma, sebaceous carcinoma, atypical fibroxanthoma, and lepromatous leprosy. In all these challenging cases, immunohistochemical investigations and integration with clinical-anamnestic information are essential for accurate classification.
Molecular Aspects and Therapeutic Implications
Recent studies have highlighted the presence of BRAFV600E mutations in BCM cases, particularly in the metastatic setting. This finding suggests that BCM, despite its unique morphology, can behave molecularly like conventional melanoma. This understanding is beginning to influence therapeutic strategies, as evidenced by recent publications.