Walking pneumonia, a term often used to describe a milder form of lung infection, can affect children and, in some instances, pose a life-threatening risk. Children diagnosed with this condition might experience significant fatigue but can often continue with many of their regular daily activities. This type of pneumonia is less common in children under the age of five.
Causes of Walking Pneumonia
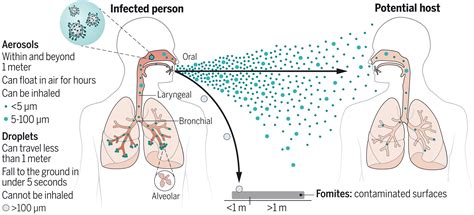
Viruses and bacteria are the primary culprits behind walking pneumonia in children. For school-aged children, the most frequent cause is the bacterium Mycoplasma pneumoniae (M. pneumoniae), which is also implicated in bronchitis and common chest colds. This bacterium spreads easily among children, especially in close proximity, such as within households, schools, or camps. Transmission occurs through airborne droplets released during sneezing, coughing, or talking, with the fall and winter months being the peak seasons for its spread.
Symptoms of Walking Pneumonia
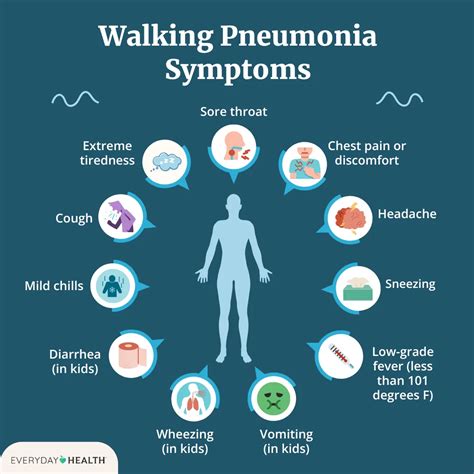
Children suffering from walking pneumonia may exhibit a range of symptoms, including:
- Fever, often low-grade
- Profound tiredness (fatigue)
- Headache
- Skin rash
- A general feeling of being unwell
- Cough, which can be dry or productive
- Ear infections
- Croup
- Sinus infections
- Sore throat
- Wheezing, particularly in children with pre-existing airway conditions like asthma
These symptoms typically manifest between one to four weeks post-exposure to the infectious agent and can persist for a week to a month.
Diagnosis of Walking Pneumonia
Healthcare providers often diagnose walking pneumonia through a physical examination and by discussing the child's symptoms. A chest X-ray is usually necessary for diagnosis. While other tests, such as blood tests, may be conducted, they are not always required.
Treatment for Walking Pneumonia
The treatment approach for walking pneumonia is tailored to the child's specific symptoms, age, overall health, and the severity and cause of the illness. If the infection is bacterial, specifically caused by M. pneumoniae, antibiotics will be prescribed. Viral infections, however, do not respond to antibiotics, and the illness must run its course.
To aid in recovery, parents are advised to ensure their child:
- Rests adequately: Ample rest helps the child's body fight the infection more effectively. A healthcare provider might recommend keeping the child home from school until symptoms improve.
- Stays hydrated: Encouraging fluid intake through water, soups, and warm teas helps prevent dehydration.
- Takes prescribed medications: Over-the-counter (OTC) medications for fever or pain may be recommended by the healthcare provider. It is crucial to discuss any OTC medication with the provider before administration, especially for the first time.
In cases of wheezing, a nebulizer might be prescribed. A cool-mist humidifier in the child's bedroom can also help alleviate breathing difficulties.
Potential Complications
Although walking pneumonia is often mild, it can sometimes lead to more serious complications, including:
- More severe forms of pneumonia
- Asthma attacks or the onset of new asthma symptoms
- Swelling of the brain (encephalitis)
- Hemolytic anemia (destruction of red blood cells)
- Kidney problems
- Skin disorders
Preventing Walking Pneumonia
While certain types of pneumonia are preventable with vaccines, no vaccine is available for infections caused by M. pneumoniae. Prevention primarily relies on good hygiene practices. Teaching children to cover their nose and mouth when coughing or sneezing, and encouraging frequent handwashing, are effective measures that also help prevent other infections.
When to Seek Medical Advice
Contact your child's healthcare provider if their symptoms worsen or do not improve. Seek immediate medical attention if your child experiences:
- Shortness of breath
- Chest pain
- High fever
Call emergency services (911) if your child exhibits:
- Severe difficulty breathing
- Blue or gray lips, nails, or skin
- Inward pulling of the skin around the ribs (retractions) during breathing
Mycoplasma pneumoniae and Extrapulmonary Manifestations
Mycoplasma pneumoniae (MP) is a common respiratory pathogen responsible for community-acquired pneumonia (CAP). Studies indicate that MP accounts for approximately 10.1% of all CAP cases, with a higher prevalence in children (17.6%) compared to adults (7.2%). A significant portion of patients diagnosed with MP, around 25%, develop extrapulmonary manifestations, which can include pericarditis, thrombosis, hepatitis, hemolytic anemia, arthritis, encephalitis, glomerulonephritis, mucositis, and various dermatologic conditions.
Mycoplasma-Induced Rash and Mucositis (MIRM)
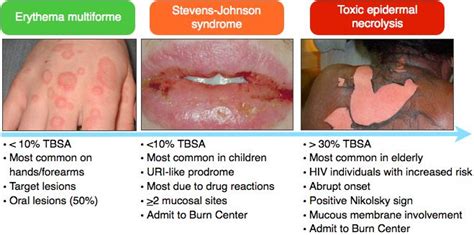
Historically, dermatologic manifestations associated with Mycoplasma pneumoniae were often categorized under erythema multiforme (EM), Stevens-Johnson Syndrome (SJS), and toxic epidermal necrolysis (TEN). However, recent research suggests these may represent a distinct disease process, termed Mycoplasma-induced rash and mucositis (MIRM). This term was coined by Canavan and colleagues in 2014 following a systematic review of 202 cases of mucocutaneous disease in patients testing positive for Mycoplasma pneumoniae. They identified a unique disease morphology that did not fit the established EM, SJS, and TEN diagnoses.
Characteristics of MIRM
MIRM is characterized by prominent mucositis (inflammation of mucous membranes) with or without cutaneous involvement. It may present with a characteristic skin vesicle or an atypical target-shaped eruption, distinguishing it from the SJS spectrum. MIRM generally follows a milder disease course with lower rates of sequelae and mortality compared to EM, SJS, and TEN. The exact pathophysiology of MIRM is still under investigation, with theories including B cell cloning with immune complex deposition and molecular mimicry between mycoplasma adhesion molecules and skin cell antigens.
Clinical Presentation of MIRM
Patients suffering from MIRM are often afflicted during winter months. The condition predominantly affects males (60-66%) and is common in young individuals (average age ranging from 8.7 to 11.9 years). Prodromal symptoms, such as fever, malaise, and cough, typically appear 7-10 days before the mucocutaneous symptoms. Cutaneous involvement can vary, with some patients exhibiting sparse lesions while others have moderate or severe involvement. Lesions are most commonly found on the extremities and can appear as vesiculobullous, targetoid, papular, macular, or morbilliform rashes.
Mucosal surface involvement is a hallmark of MIRM. The oral cavity is affected in approximately 94% of patients, with symptoms ranging from erosions and ulcers to denuded tissue. Ocular involvement, occurring in about 82% of patients, may present as purulent conjunctivitis, photophobia, pseudomembrane formation, ulceration, and eyelid edema. Urogenital lesions are reported in about 63% of patients.
Diagnosis and Treatment of MIRM
The diagnosis of MIRM is historically based on the positive identification of Mycoplasma pneumoniae through clinical, radiological, and laboratory findings, coupled with associated extrapulmonary symptoms. Proposed diagnostic criteria for classic MIRM include clinical and laboratory evidence of atypical pneumonia caused by Mycoplasma pneumoniae with at least two involved mucosal sites, less than 10% involved cutaneous surface area, and few vesiculobullous lesions or atypical scattered targets.
Treatment for MIRM primarily focuses on supportive management, including pain control, intravenous hydration, and wound care for affected mucosal surfaces. Systemic antibiotics are administered if pneumonia is confirmed. Some patients may benefit from systemic steroids to reduce inflammation, while others might receive intravenous immunoglobulins (IVIG) or cyclosporine A (CsA), particularly in severe cases. While the majority of MIRM patients recover fully, some may experience long-term sequelae, such as ocular complications or postinflammatory pigmentation changes.
Key Takeaways
- Walking pneumonia is a milder form of lung infection, often caused by Mycoplasma pneumoniae, particularly in school-aged children.
- Symptoms can include fever, fatigue, cough, and sometimes a skin rash.
- Mycoplasma pneumoniae can lead to extrapulmonary manifestations, including a distinct condition known as Mycoplasma-induced rash and mucositis (MIRM).
- MIRM involves inflammation of mucous membranes, often accompanied by characteristic skin rashes, and is distinguished from conditions like Erythema Multiforme and Stevens-Johnson Syndrome.
- Good hygiene practices, such as frequent handwashing and covering coughs/sneezes, are crucial for preventing the spread of M. pneumoniae.