The meniscus serves as a crucial fibrous shock absorber within the knee joint. Statistics from the National Center for Health Statistics indicate that tears and partial removals of the meniscus occur over a million times annually in the United States. However, surgeons opt to repair fewer than 10% of all diagnosed torn meniscus cartilages due to the inherent difficulty in repair and the variable healing history of this tissue.
The consequences of meniscus loss, such as pain and arthritis, typically manifest years later. Meniscus tears occur when the meniscus is pinched between the femur and the tibia. This can happen during sports activities, through bending or twisting motions, or even during simple actions like exiting a car. Symptoms often include a popping sensation or sudden pain, sometimes accompanied by swelling. A torn meniscus acts like a "windshield wiper" within the knee joint, causing mechanical pain and accelerating the wear of the opposing articular cartilage surface. Additionally, the cells of a torn, unstable meniscus release factors that expedite the onset of arthritis.
The Collagen Meniscus Implant (CMI), designed in 1986, functions in two primary ways. Firstly, it acts as a physical scaffold, providing a structure upon which new meniscus tissue can grow. The CMI holds the promise of opening a new avenue for meniscus reconstruction, offering an alternative to total knee replacement.
Understanding Meniscus Anatomy and Injuries
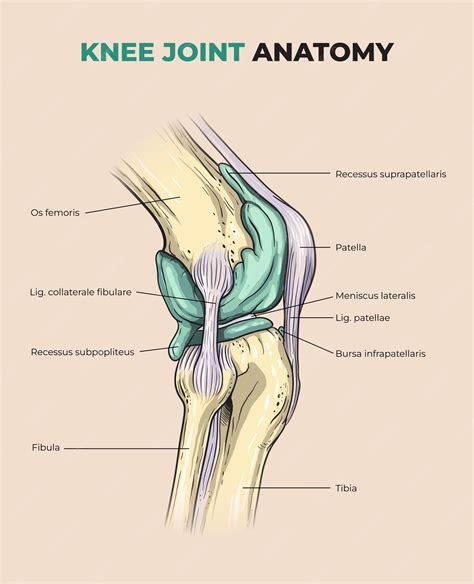
The knee menisci are wedge-shaped, semi-lunar discs of fibrous tissue situated in the knee joint between the ends of the femur and the tibia and fibula. Each knee contains a lateral and a medial meniscus.
Meniscal tears are common orthopedic injuries affecting individuals of various ages and activity levels. The incidence of meniscus injuries has been reported at 61 per 100,000 individuals. Medicare Part B claims data from 2007 identified over 125,000 meniscectomies performed on Medicare beneficiaries.
Meniscus injuries can be categorized into two main groups: traumatic tears and degenerative tears. Traumatic tears typically occur in a younger population and are usually the result of a specific traumatic event. Degenerative tears are believed to develop from intrasubstance degeneration within the menisci, often considered a part of the normal aging process.
Injuries to a healthy meniscus are induced by compressive force combined with tibiofemoral rotation in the transverse plane during movements from flexion to extension or during rapid cutting or pivoting. The pathomechanics of more complex degenerative tears remain less understood.
Historically, the meniscus was considered vestigial tissue. However, it is now recognized that the menisci provide essential mechanical support, localized pressure distribution, and lubrication to the knee joint. Initially, the primary treatment for meniscal tears was total meniscectomy. However, it was later concluded that meniscectomy is not without consequences, interfering with joint mechanics. Subsequent observations indicated that a high proportion of knees after meniscectomy showed degenerative changes, occurring more frequently than could be attributed to normal aging. As the biomechanical importance of the meniscus became apparent, it became clear that procedures preserving the meniscus offered significant long-term advantages for patients.
Complications arising from complete meniscectomy led some surgeons to adopt a more conservative approach, making partial meniscectomy the preferred technique. The definitive treatment for a meniscal tear involves repair or excision of the pathological tissue; however, not all patients with meniscal tears necessitate surgical intervention. Asymptomatic meniscal tears are relatively common findings on magnetic resonance imaging (MRI).
If a meniscus tear cannot be repaired, a conservative partial meniscectomy should be performed to preserve as much meniscal tissue as possible, thereby reducing the risk of late degenerative changes. When meniscal tears are symptomatic, patients typically report clicking and pain during activity. In some instances, a tear can displace, leading to knee joint locking.
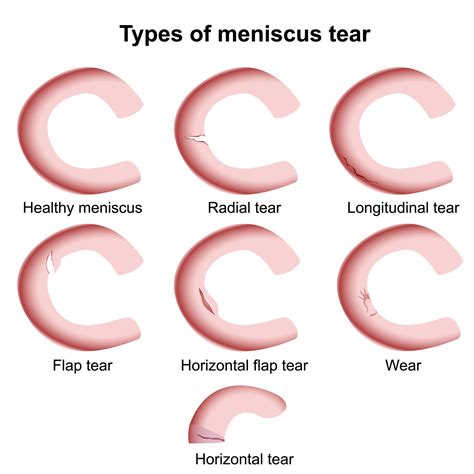
Classifying Meniscus Tears
Tear types are usually classified by the pattern of the tear. Acute tear patterns, such as vertical, bucket-handle, and radial tears, are most frequently observed in younger patients. Older patients tend to develop degenerative tear patterns, including horizontal cleavage tears, oblique tears, and complex combinations of patterns.
Tears are also classified as stable or unstable. All partial-thickness tears are considered stable. Full-thickness tears differ based on whether the tear is vertical and longitudinal, or radial. Tear types are also commonly categorized by their location relative to the peripheral blood supply, using terms such as red-red, white-white, and red-white.
- Red-red tears are peripheral and have blood supply to both sides of the tear, offering the highest chance of healing.
- White-white tears are central and avascular, presenting the least chance of healing.
- Red-white tears have vascularity on the peripheral side of the tear and no vascularity on the central side.
Treatment Controversies and Alternatives
Treatments for meniscal tears are not without controversy. Meniscectomy in older patients remains a debated topic. Arthroscopic medial meniscectomy in older patients yields good results in approximately 90% of cases six years after non-degenerative meniscal tears, but only about 20% of good results after degenerative meniscal tears. However, based on available studies, neither symptoms nor physical examination can reliably differentiate between traumatic meniscal tears and degenerative meniscal changes in older patients.
Some experts suggest that meniscus repair should be limited to patients under 50 years of age. There is still no consensus regarding the preferred treatment for degenerative meniscus tears. Studies have indicated that arthroscopic partial medial meniscectomy followed by supervised exercise is not superior to supervised exercise alone.
Research has presented limited and conflicting data on whether age, gender, and weight are significant factors influencing clinical outcomes after arthroscopic meniscal debridement. Meniscal debridement is generally reserved for unstable, symptomatic tears.
Despite advancements in understanding the physiological characteristics of knee joint menisci, these advances have not always translated into significant adjustments in clinical therapy. There is still limited evidence to suggest that newer therapeutic approaches are genuinely superior to earlier methods involving complete meniscus removal. Furthermore, there is no definitive evidence that repairing a tear in the avascular region yields better outcomes than partial meniscectomy. Results in the literature regarding whether meniscal repair leads to improved outcomes compared with meniscectomy are equivocal.
Given the recognized importance of intact menisci and the risk of developing osteoarthrosis after meniscal removal, meniscal replacement has been advocated in cases of extensive meniscal damage or after total meniscectomy. The replacement of damaged or lost portions of the meniscus cartilage is considered an appropriate approach to prevent or minimize progressive degenerative joint disease that may develop subsequently.
Understanding the Anatomy of Your Knee
The Collagen Meniscus Implant (CMI)
The Collagen Meniscus Implant (CMI) can be utilized to fill meniscal defects resulting from partial meniscectomy. It is important to note that the CMI is not designed to replace the entire meniscus, as it requires an intact meniscal rim for attachment.
The CMI is also referred to as a collagen scaffold (CS) or CMI in literature, FDA documents, and related materials. The placement of the CMI is typically performed through an arthroscopic procedure, often with an additional small incision to facilitate the capture of repair needles and the tying of sutures. Following debridement of the damaged meniscus, the implant is trimmed to match the size of the meniscal defect and then sutured into place.
The CMI is described as a tissue-engineered scaffold intended to support the generation of new meniscus-like tissue. It is manufactured from bovine collagen and should not be confused with a meniscus transplant, which involves replacing the meniscus with a donor meniscus from a cadaver.
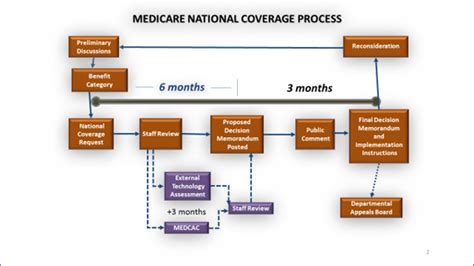
Medicare Coverage Determination
The Centers for Medicare & Medicaid Services (CMS) has concluded that the collagen meniscus implant does not improve health outcomes in the Medicare population. Consequently, CMS has determined that the collagen meniscus implant is not reasonable and necessary for the treatment of meniscal injury/tear and has issued a national non-coverage determination.
Effective for claims with dates of service performed on or after May 25, 2010, CMS determined that the available evidence is insufficient to conclude that the collagen meniscus implant improves health outcomes. Therefore, it is not considered reasonable and necessary for the treatment of meniscal injury/tear under section 1862(a)(1)(A) of the Social Security Act. In May 2010, upon completion of a national coverage analysis, the decision was made that the collagen meniscus implant is non-covered for Medicare beneficiaries.
FDA Clearance and Controversy
On December 18, 2008, the FDA provided 510(k) clearance for the ReGen Collagen Scaffold (K082079). As described in the FDA Summary, the ReGen Collagen Scaffold is a resorbable collagen matrix composed of bovine type I collagen. It is intended for use in surgical procedures for the reinforcement and repair of soft tissue injuries of the medial meniscus, requiring an intact meniscal rim and anterior and posterior horns for attachment.
The ReGen Collagen Scaffold was initially submitted to the FDA under a premarket approval application (PMA). Amid controversy surrounding the 510(K) clearance, the FDA initiated a review of the clearance process for this device. In September 2009, the FDA issued a preliminary report on its review, raising questions about the basis for the clearance decision. The FDA has undertaken a reconsideration of the decision to clear ReGenâs CS device.
Evaluating Clinical Evidence for Coverage Decisions
When making national coverage determinations, CMS evaluates relevant clinical evidence to ascertain if it is of sufficient quality to support a finding that an item or service is reasonable and necessary for the diagnosis or treatment of illness or injury, or to improve the functioning of a malformed body member. The critical appraisal of evidence helps determine the confidence in conclusively answering specific assessment questions and whether the intervention will improve health outcomes.
An improved health outcome is a key consideration in determining if an item or service is reasonable and necessary. Methodological principles of study design, such as the selection of a clinically relevant cohort, consistent use of a good reference standard, and blinding of readers to test results, improve the quality and reduce bias in clinical studies.
Public comments can provide valuable information, especially those citing published clinical evidence. Comments based on unpublished evidence, such as individual practitioner or patient results, are considered less rigorous. CMS uses initial public comments to inform its proposed decisions and responds in detail to comments on proposed decisions when issuing final decision memoranda.
Evidence for Collagen Meniscus Implants
The evidence related to the treatment of meniscus injuries with the collagen meniscus implant includes one randomized controlled clinical trial and several small case series. The focus of CMS's examination is on health outcomes, specifically the benefits and harms of a particular treatment. For meniscal injuries, the primary concern is a reduction in pain-related functional activity restriction, rather than disease and mortality outcomes.
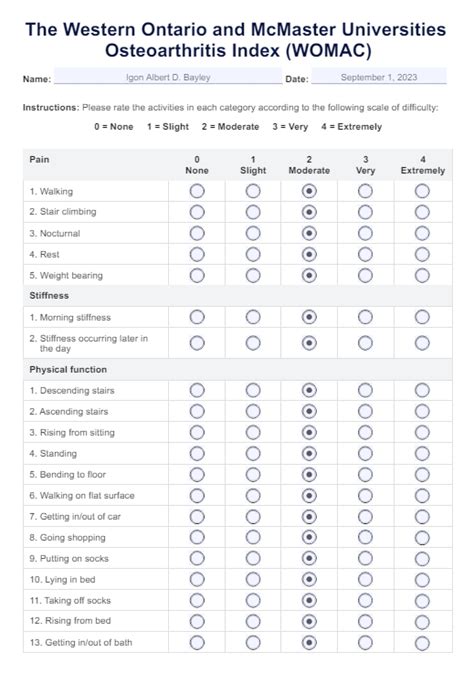
Independently assessed, validated instruments are given significant weight. For meniscal injuries, the measurement of treatment effect emphasizes patient-based quality of life instruments over clinician-based measures. Various outcome measures exist, including the Western Ontario and McMaster Universities Index (WOMAC), the Knee Injury and Osteoarthritis Outcome Score (KOOS), the Cincinnati Knee Rating System, the International Knee Documentation Committee (IKDC), and the Lysholm scale. Hop tests are also employed, particularly in anterior cruciate ligament outcome studies.
The IKDC comprises eighteen questions assessing patient symptoms and function in daily living activities and sports. Knee treatment outcomes can be graded as A (normal), B (nearly normal), C (abnormal), and D (severely abnormal). The Cincinnati Knee Rating System evaluates subjective symptoms and functional activity levels, often utilizing a portion of its comprehensive scale. The Lysholm scale is an eight-item questionnaire designed to assess patient function following knee ligament surgery.
The Role of the Meniscus and Limitations of Implants
The knee menisci are vital for mechanical support, localized pressure distribution, and lubrication of the knee joint. The collagen meniscus implant is designed to fill meniscal defects and requires an intact meniscal rim for attachment; it does not replace the entire meniscus.
The placement of the CMI is typically an arthroscopic procedure, sometimes requiring an additional small incision. After debridement of the damaged meniscus, the implant is trimmed to fit the defect and sutured in place. The CMI is considered a tissue-engineered scaffold to support the generation of new meniscus-like tissue.
Meniscal loss or dysfunction leads to abnormal wear on articular cartilage, promoting degeneration and osteoarthritis of the knee joint. Due to the limited vascularity of cartilaginous tissue, meniscus injuries may not heal effectively. The collagen meniscal implant (CMI), previously marketed as Menaflex, is derived from bovine collagen and is used to treat acute or chronic advanced meniscal loss or damage with the goal of relieving symptoms and preventing joint degeneration. It is a flexible, sickle-shaped disc attached arthroscopically to native tissue with sutures.
Meniscal replacement with CMI is indicated for patients with advanced loss or damage to meniscal tissue that cannot be repaired, provided an intact rim of meniscal tissue is present. The amount of damaged tissue must exceed 25% of the total meniscus area and extend at least into the red-white zone.
Partial meniscectomy remains the conventional treatment for meniscal tears or subtotal loss when repair is not feasible.