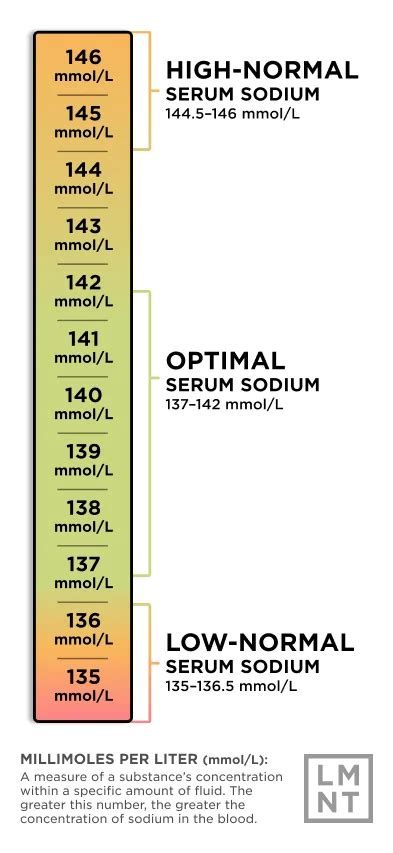
Hyponatremia is a critical electrolyte imbalance defined by a serum sodium concentration below 135 mEq/L. This condition is the most frequently encountered and significant electrolyte disturbance, occurring either independently or, more commonly, as a complication of other medical conditions such as heart failure, liver failure, kidney failure, pneumonia, and cancer. The normal serum sodium concentration typically ranges between 135-145 mEq/L. The approach to correcting hyponatremia is multifaceted, varying based on its origin, severity, and duration.
Symptoms of hyponatremia can range from mild, such as nausea and malaise, to severe, including lethargy, decreased level of consciousness, headache, and in pronounced cases, seizures and coma. The onset can be either acute (less than 48 hours) or chronic (greater than 48 hours). For patients with chronic hyponatremia (duration exceeding 48 hours), treatment must be carefully managed to prevent osmotic demyelination syndrome (ODS), a serious neurological complication that can arise from overly rapid correction of serum sodium levels.
Etiology and Classification of Hyponatremia
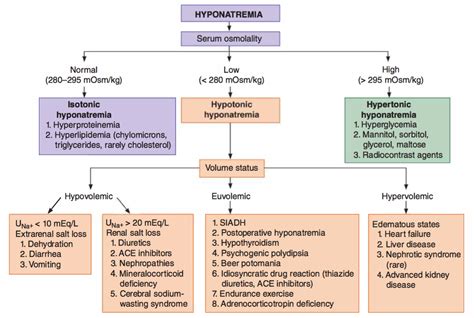
Hyponatremia is classified based on serum osmolality and extracellular volume status, with multiple underlying etiologies often contributing. The most frequent causes of hyponatremia encountered in emergency departments include the use of thiazide diuretics and the syndrome of inappropriate antidiuretic hormone secretion (SIADH). Exercise-associated hyponatremia is particularly noted in endurance athletes, such as marathon runners, but also in other strenuous activities like football, cycling, and military training.
Pseudohyponatremia, an artifactual low serum sodium level, can occur in conditions with very high protein (e.g., multiple myeloma) or glucose levels (e.g., diabetic ketoacidosis - DKA) in the blood. In these situations, the measured sodium concentration is falsely low due to alterations in the plasma water fraction. Severe hyperlipidemia and paraproteinemia can also lead to low measured serum sodium concentrations despite normal serum osmolality. This artifact is often due to measurement by flame photometry and can be avoided by direct ion-selective electrode measurement. Another cause of pseudohyponatremia involves patients with cholestatic jaundice due to the presence of low-density lipoprotein, lipoprotein X, which can be identified through lipoprotein electrophoresis.
Hyponatremia following transurethral resection of the prostate (TURP) or hysteroscopy is attributed to the absorption of nonconductive irrigating solutions like glycine, sorbitol, or mannitol. The severity of hyponatremia correlates with the volume and rate of fluid absorption. Hemodialysis can be employed to correct hyponatremia and remove glycine and its metabolites in patients with end-stage renal disease. The use of isotonic saline as an irrigant instead of glycine in modern TURP procedures for high-risk patients can help prevent this complication, making it a less common diagnosis today.
Key Diagnostic Tests
Three essential laboratory tests aid in evaluating patients with hyponatremia:
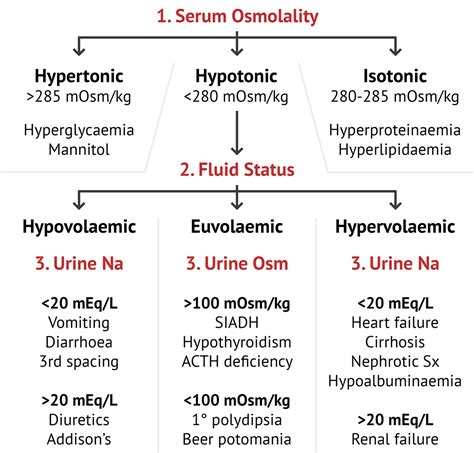
- Serum osmolality: This test is crucial for differentiating true hyponatremia (hypotonic hyponatremia) from pseudohyponatremia.
- Urine osmolality: Helps distinguish between conditions with and without antidiuretic hormone (ADH), also known as arginine vasopressin (AVP). A dilute urine (urine osmolality < 100 mOsm/kg) with hypotonic hyponatremia typically arises from conditions overwhelming the kidney's free water excretion capacity (e.g., primary polydipsia) or from a low solute load (e.g., a "tea and toast" diet). A urine osmolality greater than 100 mOsm/kg suggests an impaired ability of the kidneys to dilute urine, usually due to physiological or non-physiological ADH secretion.
- Urinary sodium concentration: Assists in differentiating hyponatremia secondary to hypovolemia or ineffective intravascular volume from SIADH. In SIADH and salt-wasting syndromes, urine sodium is typically greater than 20-40 mEq/L. In hypovolemia or ineffective intravascular volume states, urine sodium is usually less than 20 mEq/L.
Pathophysiology and Clinical Features
The clinical manifestations of hyponatremia are contingent upon its onset, duration, and severity. Most individuals with chronic hyponatremia remain asymptomatic, with symptoms typically manifesting only when serum sodium concentration drops below 120 mEq/L. Symptoms usually develop acutely (onset < 48 hours) or slowly (onset > 48 hours) and are often nonspecific.
Hypotonic hyponatremia, which accounts for the majority of clinical cases, necessitates free water restriction. Acute hyponatremia (duration < 48 hours) can be corrected more rapidly than chronic hyponatremia. For patients with overt symptoms, such as seizures or severe neurological deficits, and generally those with severe hyponatremia, treatment involves a hypertonic (3%) saline bolus to elevate serum sodium concentration and alleviate symptoms. Moderate symptoms may warrant a slow infusion of hypertonic saline. Isotonic saline is administered to hypovolemic patients to restore intravascular volume. Patients with diuretic-induced hypovolemia may also require potassium repletion. Hypervolemic patients are typically managed with fluid restriction, potentially with loop diuretics, and treatment of the underlying condition. For asymptomatic patients with euvolemic hyponatremia, free water restriction is the primary treatment modality.
Osmotic demyelination syndrome (ODS) is a serious risk associated with the overly rapid correction of chronic hyponatremia. To mitigate this risk, sodium concentration should ideally be increased by 4-6 mEq/L within the first 1-2 hours for patients experiencing severe or moderately severe symptoms, or those with acute hyponatremia. Serum sodium levels require monitoring every 6-8 hours in patients receiving vaptan therapy to prevent overcorrection. If hyponatremia persists after discontinuing diuretic use, other underlying causes should be investigated.
Central Pontine Myelinolysis | Osmotic Demyelination Syndrome
Calculated Serum Osmolality and Hyperglycemia
Serum osmolality can be calculated using the formula: 2(Na+ mEq/L) + serum glucose (mg/dL)/18 + BUN (mg/dL)/2.8. This calculation is important because glucose can lower the serum sodium level. Specifically, glucose reduces serum sodium by approximately 1.6 mEq/L for every 100 mg/dL of serum glucose exceeding 100 mg/dL. A more accurate correction factor of 2.4 mEq/L for each 100 mg/dL increase over 100 mg/dL is used when glucose levels are greater than 400 mg/dL, as the relationship becomes non-linear at higher concentrations.
Hypo-osmolality (serum osmolality < 275 mOsm/kg) consistently indicates an excess of total body water relative to body solutes or an excess of water within the extracellular fluid (ECF), given that water freely moves between intracellular and extracellular compartments. Under normal physiological conditions, the kidneys are capable of excreting substantial amounts of free water, up to 15-20 liters per day. Concurrently, the body's response to decreased osmolality includes a reduction in thirst.
Specific Causes and Management Strategies
SIADH is a common cause of hyponatremia, characterized by impaired water excretion due to the inappropriate secretion of ADH. In SIADH, urinary sodium concentrations are typically greater than 20-40 mEq/L. Management often involves fluid restriction. Another important, though rare, cause of normovolemic hypotonic hyponatremia is a reset osmostat, which can be observed in the elderly and during pregnancy.
Severe hypothyroidism (mechanism unclear, possibly related to low cardiac output and glomerular filtration rate) and adrenal insufficiency are also linked to non-osmotic vasopressin release and impaired sodium reabsorption, leading to hypotonic hyponatremia. Hyponatremia associated with cortisol deficiency, such as primary or secondary hypoadrenalism, may present subtly and go undiagnosed. A random cortisol level check during acute illness can be misleading if it is normal when it should be elevated.
Patients infected with human immunodeficiency virus (HIV) exhibit a high incidence of hyponatremia, often due to adrenal insufficiency, potentially caused by infections like cytomegalovirus or Mycobacterium avium-intracellulare. These patients may present with signs of solute depletion and orthostatic symptoms.
The pathophysiology of hypovolemic hypotonic hyponatremia is complex, involving interactions between carotid baroreceptors, the sympathetic nervous system, the renin-angiotensin system, ADH secretion, and renal tubular function. Increased sympathetic tone and reduced renal perfusion due to intravascular volume depletion stimulate renin and angiotensin secretion, leading to increased sodium absorption in proximal tubules and impaired free water excretion. Concurrently, increased serum ADH production further hinders free water excretion. Angiotensin also stimulates thirst, leading to inappropriate increased free water intake when water excretion is already limited.
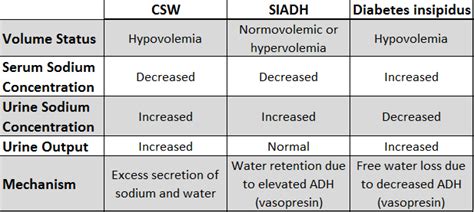
Cerebral salt wasting (CSW) is observed in patients with intracranial disorders such as subarachnoid hemorrhage, meningitis, traumatic brain injury, and pituitary disorders, particularly after neurological procedures. In CSW, plasma renin and aldosterone levels may not rise appropriately despite reduced plasma volume due to disruption of the sympathetic nervous system. The renal salt wasting in CSW might also be influenced by natriuretic factors. Distinguishing CSW from SIADH can be challenging due to overlapping clinical presentations. Vigorous salt replacement is crucial for CSW, whereas fluid restriction is the mainstay for SIADH. Isotonic saline infusion to correct volume depletion is often effective in reversing hyponatremia in CSW, as euvolemia suppresses ADH release.
Diuretics can precipitate hypovolemic hyponatremia. Thiazide diuretics, unlike loop diuretics, impair urine dilution without affecting concentration, thereby hindering free water excretion and posing a higher risk for hyponatremia. The most common precipitating factor for hyponatremia in postoperative patients is the iatrogenic infusion of hypotonic fluids.
In severely malnourished individuals with a low-protein, high-water diet, diminished solute intake limits the kidney's ability to excrete free water, similar to the condition known as beer potomania. Compulsive intake of large volumes of water exceeding the kidneys' diluting capacity (> 20 L/d), even with normal solute intake, can lead to hyponatremia. These individuals will excrete maximally dilute urine (urinary osmolality < 100 mOsm/kg), distinguishing them from patients with SIADH.
Primary polydipsia involves a defect in thirst regulation, often associated with psychiatric illness, and may involve abnormalities in ADH regulation. Factors contributing to hyponatremia in these patients include transient ADH release during acute psychotic episodes, increased renal response to ADH, downward resetting of the osmostat, and the effects of antipsychotic medications. Limiting water intake can rapidly normalize plasma sodium levels as excess water is efficiently excreted.
Acute hyponatremia is not uncommon in ultra-endurance athletes and marathon runners, with women being at higher risk. The strongest predictor of hyponatremia in these cases is weight gain during the event, correlating with excessive fluid intake. Longer race times and extreme low body mass index are also associated factors, while the type of fluid consumed (plain water versus electrolyte-containing sports drinks) is less critical. Some athletes may be normonatremic or even hypernatremic, underscoring the complexity of blanket recommendations. However, fluid intake leading to weight gain should be avoided. Athletes are advised to rely on thirst as their guide for fluid replacement and refrain from adhering to universal water intake guidelines.
For symptomatic patients with documented hyponatremia, immediate administration of 100 mL of 3% sodium chloride over 10 minutes in the field, prior to hospital transportation, may be considered to help manage symptoms.
Tolvaptan, an oral selective vasopressin V2 receptor antagonist, is indicated for hypervolemic and euvolemic hyponatremia. Conivaptan, an intravenous V1A and V2 vasopressin receptor antagonist, is approved for hospital use in euvolemic and hypervolemic hyponatremia.
tags: #hyponatremia #serum #osmolality