Clotrimazole is a synthetic imidazole with a broad spectrum of antimycotic activity, making it a prominent antifungal medication widely used to treat various fungal infections. It is an FDA-approved drug for treating oral candidiasis, vulvovaginal candidiasis, and dermatomycoses. Additionally, clotrimazole is an effective treatment for skin infections such as athlete's foot, jock itch, ringworm, pityriasis versicolor, intertrigo, and erythrasma. The drug also exhibits some activity against certain gram-positive bacteria and, at very high concentrations, against Trichomonas spp.
In adults and children older than 12, clotrimazole in combination with betamethasone propionate (a corticosteroid) is approved for the topical treatment of inflammatory tinea caused by Epidermophyton floccosum and Trichophyton. However, caution is advised as such combinations can sometimes aggravate fungal infections.
Mechanism of Action
Interference with Ergosterol Biosynthesis
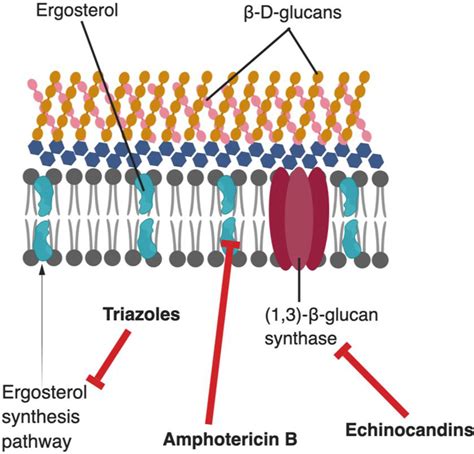
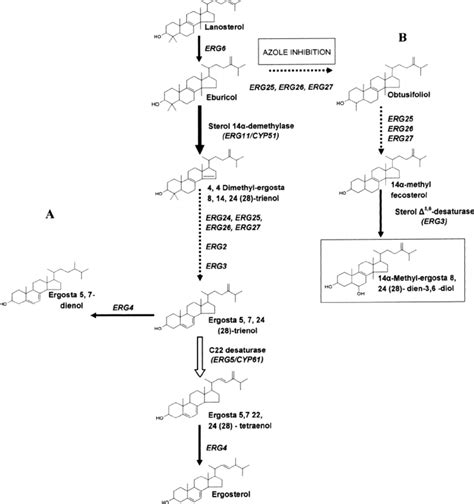
Clotrimazole exerts its primary antifungal action by damaging the permeability barrier in the fungal cytoplasmic membrane. It achieves this by inhibiting the biosynthesis of ergosterol, a crucial component of fungal cell membranes, in a concentration-dependent manner. Specifically, clotrimazole inhibits the demethylation of 14-α-lanosterol, a key step in the ergosterol pathway.
Ergosterol is essential for the structure and function of the fungal cytoplasmic membrane, analogous to cholesterol's role in human cell membranes. By blocking ergosterol synthesis, clotrimazole compromises the cell's ability to construct an intact and functional cell membrane. This disruption leads to increased membrane permeability, allowing essential intracellular components to leak out and harmful substances to enter the cell, ultimately resulting in cell death.
Concentration-Dependent Inhibition
The interference with ergosterol synthesis is concentration-dependent. At low concentrations, clotrimazole exhibits a partially inhibitory effect on ergosterol biosynthesis. However, at high concentrations, it can completely block ergosterol synthesis. This leads to a corresponding reduction in fungal growth and, with prolonged incubation, can result in fungicidal action due to ergosterol depletion.
Effects on Fungal Growth and Cell Processes
The depletion of ergosterol and the accumulation of toxic intermediates in the fungal cell membrane have several detrimental effects. Beyond compromising membrane integrity, the disruption impacts the function of membrane-bound enzymes and receptors. This hinders vital cellular processes such as nutrient uptake, ion regulation, and signal transduction, further impairing the fungus's ability to survive and proliferate.
Ergosterol also directly promotes the growth of fungal cells in a hormone-like fashion. Therefore, the rapid onset of these events-ergosterol depletion and membrane disruption-leads to a dose-dependent inhibition of fungal growth.
Differential Susceptibility
An interesting characteristic of azole antifungals, including clotrimazole, is the differential susceptibility observed between various fungal forms. Hyphae and pseudomycelia of Candida albicans are significantly more susceptible to azoles than yeast cells. Even 1% of the minimum inhibitory concentration of clotrimazole can totally inhibit mycelial growth in vitro. This observation may have clinical importance, as hyphal germination has been reported to enhance the adherence of Candida albicans.
Pharmacological Properties and Administration
Spectrum of Activity
Clotrimazole exhibits broad-spectrum antifungal activity, making it effective against a wide range of fungal pathogens, including Candida species, dermatophytes, and various molds. This versatility stems from its ability to target a fundamental aspect of fungal biology-the cell membrane-which is common across diverse fungal species.
Formulations and Administration Routes
Clotrimazole is available in various formulations for different routes of administration:
- Oral lozenges (troches): Used for local treatment of oropharyngeal candidiasis. These are administered transmucosally and do not demonstrate significant systemic bioavailability. Patients should allow the troches to dissolve slowly in their mouths without chewing.
- Topical formulations: Available as creams, ointments, lotions, and solutions (1%). These are applied by gently rubbing the medication into the cleansed, affected skin. Topical preparations should not be used in the eye or intravenously.
- Intravaginal formulations: Available as creams (1% and 2%) and tablets. These are used for the treatment of vulvovaginal candidiasis. Some products are available in combination packages with intravaginal cream and tablets. The intravaginal cream may be applied externally to the vulva to relieve itching and discomfort. Special applicators may be provided by the manufacturer.
Absorption and Bioavailability
Clotrimazole demonstrates poor absorption after dermal and intravaginal administration. Following topical application, there is minimal systemic absorption. Approximately 3% to 10% of the dose is absorbed through the intravaginal route, with vaginal cream reaching peak serum levels in about 24 hours. Fungicidal concentrations can persist in the vagina for up to 3 days after application.
Clinical Indications and Dosage
Fungal Skin Infections
- Tinea pedis (athlete's foot), Tinea corporis (ringworm), Tinea cruris (jock itch): Topical cream, solution, or lotion (1%) should be applied to the affected skin and surrounding areas twice daily. Treatment should continue for 1 week after clinical resolution.
- Cutaneous candidiasis: Topical cream, solution, or ointment (1%) should be applied to the affected area twice daily. If no improvement occurs after 4 weeks of therapy, the diagnosis should be re-evaluated.
- Pityriasis versicolor: Topical application to the affected skin and surrounding areas twice daily.
- Intertrigo: Topical application as needed.
Candidiasis
- Vulvovaginal candidiasis (VVC): Intravaginal application of 1% cream (one applicatorful, 50 mg) vaginally for 7 days, or 2% cream (one applicatorful, 100 mg) vaginally at bedtime for 3 days. For active infections, 10 mg is slowly dissolved in the mouth 5 times daily for 7 to 14 days.
- Oropharyngeal candidiasis (thrush): Transmucosal application of 10 mg lozenges, dissolved slowly in the mouth 5 times daily for 7 to 14 days.
How to use Low Dose Vaginal Estradiol
Special Populations and Considerations
Pregnancy and Breastfeeding
Clotrimazole is generally considered safe for topical use during pregnancy, particularly in the second and third trimesters. However, it should only be used if indicated during the first trimester. Clinical trials have shown intravaginal clotrimazole to be safe during the second and third trimesters. According to CDC guidelines, only topical azole therapies for 7 days are recommended for pregnant women with VVC. Clotrimazole is not known to cross the placenta, and no teratogenic effects have been demonstrated in human studies. In animal studies, high doses were embryotoxic. For breastfeeding mothers, topical clotrimazole poses little risk to nursing infants due to minimal maternal absorption. However, mothers should be instructed not to apply clotrimazole topically to the breast during breastfeeding. Oral troches should be used cautiously as they may be systemically absorbed.
Pediatric Use
Dosage regimens for children and adolescents are available for various indications, including VVC, oropharyngeal candidiasis, and tinea versicolor. For oropharyngeal candidiasis in children and adolescents aged 3 to 17, 10 mg PO 5 times daily for 7 to 14 days is recommended. For VVC in adolescent females aged 12 to 17, specific intravaginal application guidelines apply.
Hepatic Impairment
The manufacturer's labeling does not provide specific dosage adjustments for hepatic impairment. However, caution should be exercised, as abnormal liver function test (LFT) elevations have been reported, particularly with oral formulations.
Immunocompromised Patients and Recurrent Infections
Guidelines recommend a treatment duration of 7 to 14 days for immunocompromised patients and recurrent infections.
Adverse Effects and Drug Interactions
Common Adverse Effects
Adverse effects can vary depending on the formulation and route of administration:
- Oral formulation: Itching, nausea, and vomiting. More than 10% of patients may experience abnormal liver function tests, necessitating periodic monitoring.
- Intravaginal use: Less than 10% of patients may experience a vulvar or vaginal burning sensation.
- Topical use: Rash, hives, blisters, burning, itching, peeling, redness, swelling, pain, or other signs of skin irritation.
Significant Drug Interactions
Clotrimazole therapy may result in a significant rise in tacrolimus levels, potentially leading to tacrolimus-associated toxicities. Caution should be exercised when co-administering these medications. Vaginal antifungal agents may reduce the therapeutic effectiveness of progesterone.
Contraindications and Precautions
- Hypersensitivity: Patients with hypersensitivity to clotrimazole or other azole antifungals should avoid its use.
- Ocular exposure: If eye contact occurs, the affected eye should be flushed immediately with cool, clean water.
- Systemic infections: Clotrimazole is not suitable for the treatment of systemic fungal infections.
- Onychomycosis: Topical clotrimazole is not effective for fungal infections of the nails.
- Contraceptive devices: Intravaginal clotrimazole preparations can damage contraceptive devices such as diaphragms, condoms, and cervical caps, potentially leading to contraceptive failure. Patients should abstain from sexual intercourse during treatment and use alternative birth control methods.
Monitoring and Healthcare Team Collaboration
Monitoring Parameters
For patients receiving oral clotrimazole (troche), periodic monitoring of liver function tests is recommended due to the potential for abnormal LFT elevations. Patients should be monitored for any hypersensitivity or local irritation, especially with topical and intravaginal applications.
Enhancing Healthcare Outcomes
Careful evaluation and reassessment are crucial before prescribing or dispensing clotrimazole, especially with atypical symptoms. Vaginal candidal infections can co-exist with other sexually transmitted diseases. Symptoms such as foul-smelling vaginal discharge, abdominal pain, or fever higher than 100 °F (37.8 °C) may indicate other vaginal infections or pelvic inflammatory disease. Healthcare providers should counsel patients on the importance of reading labels, understanding potential side effects, and avoiding drug-related toxicities due to overdosing. Pharmacists should check for drug interactions and inform prescribers and patients of any concerns. Interprofessional collaboration among clinicians, nurses, physician assistants, and pharmacists is essential for optimizing antifungal treatment, identifying warning signs of serious illness, and improving patient outcomes.
tags: #mechanism #of #action #of #clotrimazole