Survival rates offer an estimation of the percentage of individuals diagnosed with a specific type and stage of cancer who remain alive after a defined period, typically five years. It is crucial to understand that these rates are statistical estimates derived from the outcomes of large patient groups with similar diagnoses. They cannot predict the course of the disease for any particular individual. These statistics can sometimes be confusing and may prompt further questions.
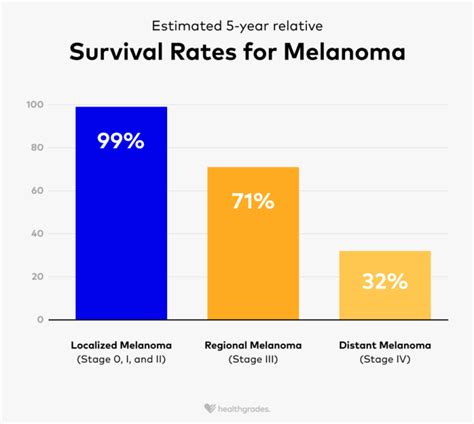
A relative survival rate compares individuals with a specific cancer to the general population. The Surveillance, Epidemiology, and End Results (SEER) database in the United States tracks 5-year relative survival rates for melanoma skin cancer based on the extent of cancer spread. However, the SEER database does not categorize cancers by the American Joint Committee on Cancer (AJCC) TNM stages. The provided survival statistics apply solely to the stage of cancer at the time of initial diagnosis and do not encompass all influencing factors. While survival rates are based on the extent of cancer spread, an individual's age, overall health, response to treatment, and other personal factors significantly impact their prognosis.
For instance, younger individuals generally have a more favorable outlook than older individuals, irrespective of the cancer stage. It is also important to note that individuals diagnosed with melanoma today may have a better prognosis than these historical statistics suggest.
Understanding Scalp Melanoma
Often referred to as the “invisible killer,” skin cancer of the scalp is a prevalent form of skin cancer, largely due to its high exposure to the sun. While various types of skin cancer can manifest on the scalp, melanoma stands out as the deadliest and one of the most common. Astonishingly, the scalp accounts for over 49% of all melanoma sites. The incidence of melanoma has been on the rise, increasing at a rate of 5% annually, as reported by the NCBI in 2020, a rate higher than most other cancers except for lung cancer in women.
According to the American Cancer Society, individuals with fair skin, freckles, and lighter hair are at the highest risk of developing melanoma compared to those with different skin and hair types. People with Fitzpatrick skin type I have an ivory skin tone that tends to freckle and burn easily without tanning when exposed to the sun. Those with Fitzpatrick skin type II have a fair to beige complexion that may occasionally tan, burn, or freckle. Both of these skin types are at a heightened risk of premature skin aging and sun damage.
Risk Factors for Scalp Melanoma
Exposure to ultraviolet radiation (UVR), including that from indoor tanning devices, is believed to contribute to melanoma development, with each tanning session increasing a patient's risk.
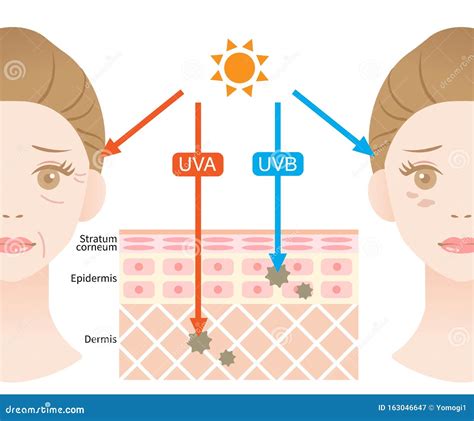
- UVA light: This type of light, present in natural sunlight, is thought to cause oxidative DNA damage, as noted in a 2020 NCBI report. While UVA rays are more prevalent in sunlight than UVB rays, standard sunscreen SPF ratings only account for UVB protection. Therefore, it is essential to take extra precautions during prolonged sun exposure, particularly if you are prone to sunburn. Look for "broad-spectrum protection" on sunscreen labels, as these formulations consider UVA light.
- UVB light: UVB light is considered the primary cause of intense DNA damage to the skin. The Skin Cancer Foundation indicates that UVB light is mainly associated with sunburn and damages the outermost layers of the skin.
Increased sun exposure has significant implications for scalp cancer. A 2020 study analyzing 113 primary scalp melanomas over 20 years in Australia and Italy found that 70% of these melanomas occurred on sun-damaged scalps. Furthermore, 86% of these scalp melanomas were identified in men. A study published in the American Cancer Society's journal Cancer corroborated this finding.
In 2020, a study published in Cancer Epidemiology Biomarkers & Prevention examined 4,480 melanoma cases from the Western Australian Melanoma Health Study (WAMHS) and the Genes, Environment, and Melanoma (GEM) study. This research revealed a significant increase in the incidence of developing superficial spreading melanoma (SN melanoma) with each additional copy of the minor T allele of the IRF4 SNP rs12203592. Additionally, a 2020 NCBI report stated that atypical mole syndrome, caused by a defect in the CDKN2A gene responsible for the transcription factor p16 (involved in apoptosis) and p14ARF, increases the risk of melanoma.
Prognosis and Survival Rates for Scalp Melanoma
Mohs micrographic surgery offers a high success rate of up to 99% for treating skin cancer, though its application on the scalp can be more complex. The following statistics are based on large patient cohorts and should be considered estimates, not definitive predictions for individual cases.
The terms "1-year survival" and "5-year survival" do not imply a lifespan limited to one or five years. Health organizations and researchers collect data over time to assess outcomes for individuals diagnosed with cancer. While 5-year survival is a common benchmark, many patients live considerably longer. 5-year survival refers to the percentage of individuals who have not died from their cancer within five years of diagnosis.
Survival by Stage (England Data, 2013-2017 Diagnoses)
While UK-wide statistics for melanoma survival by stage are not uniformly available, survival statistics for each stage of melanoma in England have been compiled. These figures represent men and women diagnosed between 2013 and 2017.
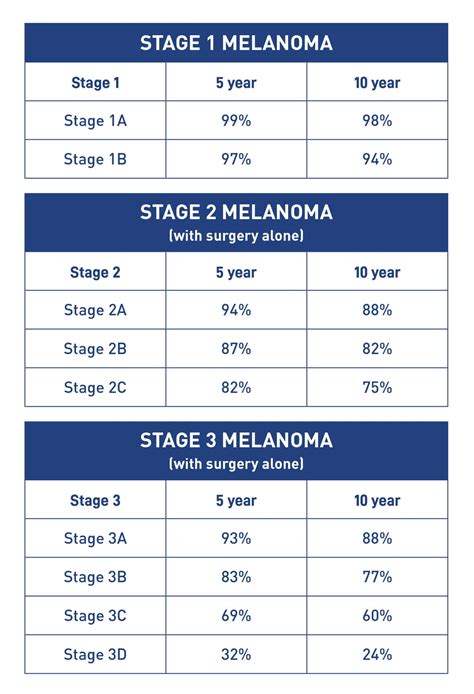
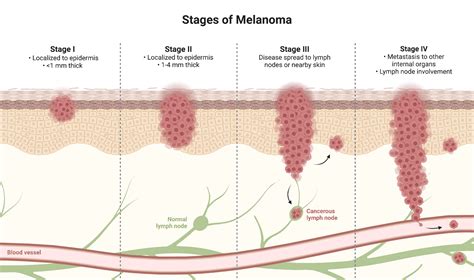
- Stage 1: Almost all individuals (around 100%) diagnosed with stage 1 melanoma skin cancer survive for five years or more.
- Stage 2: Approximately 85 out of 100 people (around 85%) with stage 2 melanoma skin cancer survive for five years or more after diagnosis.
- Stage 3: Nearly 75 out of 100 people (almost 75%) diagnosed with stage 3 melanoma skin cancer survive for five years or more.
- Stage 4: In recent years, significant advancements in treatment for stage 4 melanoma have been made, particularly with immunotherapy. Some patients are experiencing prolonged survival with stage 4 melanoma, with some even achieving long-term remission. However, this is not universally the case, and survival durations vary.
NHS England provides survival statistics for stage 4 melanoma, but these do not fully reflect outcomes for patients who have received the newest treatments, as it takes time to gather comprehensive data on these advancements.
Survival Rates with Advanced Immunotherapy Treatments
Statistics from a worldwide study involving 945 individuals with advanced melanoma (stage 3 or 4) who received immunotherapy drugs like nivolumab (Opdivo), ipilimumab (Yervoy), or a combination, offer insights:
- Patients were followed for six and a half years.
- The study also compared survival rates between patients with specific gene mutations (BRAF V600 positive) and those without (BRAF negative or wildtype).
For individuals receiving a combination of nivolumab and ipilimumab:
- BRAF-positive melanoma: More than 55 out of 100 people (over 55%) survived for six and a half years or longer.
- BRAF-negative melanoma: Around 45 out of 100 people (around 45%) survived for six and a half years or longer.
Overall Survival for All Stages (UK)
UK survival statistics, primarily derived from England and Wales, are generally applicable to Scotland and Northern Ireland due to similar population and healthcare systems.
- 1-year survival: Almost 100 out of every 100 adults (nearly 100%) with melanoma skin cancer survive for one year or more.
- 5-year survival: Approximately 95 out of every 100 adults (around 95%) survive for five years or more.
- 10-year survival: Around 95 out of every 100 adults (approximately 95%) survive for ten years or more.
Factors Influencing Survival
An individual's prognosis is influenced by several factors:
- Stage of cancer: The depth of tumor growth and whether it has spread to lymph nodes or distant organs at the time of diagnosis.
- Type of melanoma: Different subtypes of melanoma have varying prognoses.
- Anatomic site: The location of the melanoma on the body.
- Treatment received: The type of treatment administered.
- Treatment efficacy: How well the treatment works for the individual.
- General health and fitness: The patient's overall physical condition.
Notably, survival rates for melanoma are generally better for women than for men, although the exact reasons for this difference are not fully understood.
Specific Considerations for Scalp Melanoma
Melanoma of the scalp, while comprising a small percentage of all cutaneous melanomas (3-5%), has historically presented unique challenges and poorer prognoses compared to melanomas on other body parts. Research utilizing large datasets, such as the SEER program, has aimed to clarify the prognostic significance of tumor location, particularly for the scalp and neck region.
SEER Program Data Analysis (1992-2003)
An analysis of SEER data from 1992 to 2003, focusing on 51,704 cases of first invasive cutaneous melanomas among white, non-Hispanic adults, revealed significant differences. Patients with scalp/neck melanomas were found to be older (mean age at diagnosis 58.8 years vs. 55.1 years for other sites), presented with thicker tumors (median thickness 0.80 mm vs. 0.63 mm), and were more likely to be male (74% vs. 54%). Additionally, scalp/neck melanomas showed a higher incidence of ulceration (7% vs. 5%), positive lymph nodes (7% vs. 4%), and were more frequently classified as nodular melanoma (NM) or lentigo maligna melanoma (LMM).
Bivariate analyses indicated that scalp/neck melanomas were associated with a significantly higher risk of melanoma-related death. Fourteen percent of individuals with scalp/neck melanoma died from the disease, compared to 6% with extremity melanomas, 8% with trunk melanomas, and 6% with face/ear melanomas. This disparity persisted even after adjusting for age, sex, Breslow thickness, and ulceration in a multivariate Cox model. Patients with scalp/neck melanoma had approximately 1.84 times the rate of melanoma-specific death compared to those with extremity melanomas. This increased risk remained significant even after controlling for lymph node status and excluding cases of LMM or NM.
Patients with melanomas on the trunk showed an intermediate survival rate between those with scalp/neck melanomas and extremity melanomas.
Key findings from SEER data regarding scalp/neck melanomas:
- Represented 6% of all melanomas but accounted for 10% of melanoma deaths.
- More likely to occur in older males.
- Tended to be thicker, ulcerated, and classified as LMM or NM.
- Associated with positive lymph nodes.
- Carried nearly double the rate of melanoma-specific death compared to extremity melanomas, even after statistical adjustments.
Recent Studies on Scalp Melanoma
More recent studies continue to highlight the particular challenges associated with scalp melanoma. One study involving 250 non-metastatic patients who underwent wide local excision for primary scalp melanoma between 1998 and 2010 reported the following 5-year survival rates:
- Stage I: 86%
- Stage II: 57%
- Stage III: 45%
Five-year scalp control rates were also reported:
- Stage I: 92%
- Stage II: 75%
- Stage III: 63%
Recurrence was observed in 74 patients (30%), with the site of recurrence being isolated to the scalp in 23 patients (31%), neck in 12, distant sites in 22, and multiple regions in 17.
Another retrospective analysis of 93 patients with scalp melanoma compared to 1076 patients with melanomas on other sites found:
- Scalp melanomas were more frequent in male patients (79.6% vs. 52.0%).
- They tended to have nodular histology (41.1% vs. 29.2%) with a higher mitotic rate.
- While not significantly associated with other histopathological parameters like Breslow thickness or ulceration, scalp melanomas were associated with poorer survival outcomes.
- The median survival time for scalp melanomas was 15.6 months, with a 5-year recurrence-free survival of 45.1%, compared to 23.5 months and 63.6% for other sites, respectively.
- The median overall survival time was 25.6 months with a 5-year overall survival rate of 44.1% for scalp melanomas, versus 28.7 months and 62.9% for other sites.
These findings underscore that scalp melanoma, despite its relatively small proportion of all melanomas, often presents with more aggressive characteristics and a worse prognosis, frequently going undetected longer due to its location and hair coverage.
ABCDE Melanoma Skin Cancer Assessment Nursing (with Pictures)
Signs and Symptoms of Scalp Melanoma
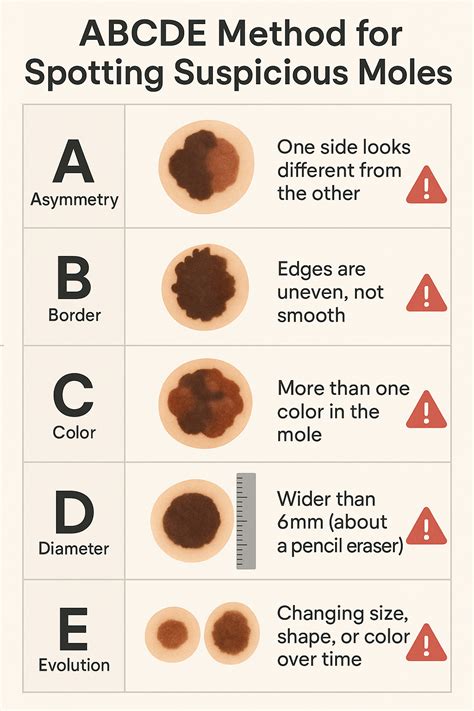
The warning signs of a suspicious mole on the scalp are consistent with those to watch for on other parts of the body. While many moles are benign, any new or changing mole should be evaluated. The ABCDE rule is a helpful guide:
- Asymmetry: One half of the mole does not match the other.
- Border irregularity: The edges are jagged, notched, or blurred.
- Color variation: The mole displays multiple colors or uneven pigmentation.
- Diameter: The mole is larger than a pencil eraser (approximately 6 millimeters or 0.25 inches).
- Evolving: The mole changes in color, shape, or texture over time.
Due to hair coverage, it is often beneficial to have a loved one assist with regular scalp skin checks to ensure thoroughness.
Diagnosis and Treatment
Diagnosis typically begins with a visual examination by a dermatologist, followed by a biopsy of any suspicious lesion. The stage of the melanoma is determined by its depth, involvement of lymph nodes, and potential spread to distant organs. Imaging tests may be recommended if the melanoma is deep or has spread.
Treatment options for scalp melanoma depend on the stage and extent of the disease. Early-stage melanomas that have not spread are typically removed surgically with wide margins. If lymph nodes are involved, they may be surgically removed. For more advanced cases, treatment may include immunotherapy, radiation therapy, or chemotherapy.