Both paronychia and felon are common infections affecting the distal parts of the fingers. While they share some similarities, they differ significantly in their depth and location. Understanding these differences is crucial for timely and effective treatment, which can prevent the spread of infection to more serious structures like bones, joints, or tendons.
Understanding Paronychia
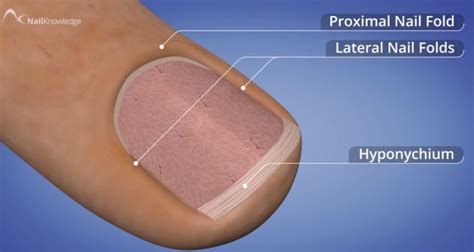
Paronychia is an infection or inflammation of the nail folds, specifically the lateral or proximal nail folds surrounding the fingernail or toenail. It's one of the most prevalent infections of the hand.
Causes and Pathophysiology of Paronychia
Paronychia arises from a disruption of the protective barrier between the nail and its surrounding fold, often due to minor trauma. This breach allows bacteria or fungi to enter, leading to infection.
Acute Paronychia
Acute cases typically develop rapidly, often within days, and are usually caused by bacterial infections. The most common culprit is Staphylococcus aureus, frequently entering through minor trauma such as hangnails, cuticle damage from manicures, or nail biting.
Chronic Paronychia
Chronic paronychia persists for more than six weeks and is often associated with recurrent inflammation. It commonly involves fungal infections, particularly Candida albicans, and can also be linked to irritant exposure from prolonged contact with water or chemicals. Conditions like dermatitis also predispose individuals to chronic paronychia.
Risk Factors for Paronychia
- Nail biting
- Aggressive manicuring or pedicuring
- Application of artificial nails
- Ingrown nails
- Minor trauma to the nail fold
- Recurrent exposure to water or chemicals (e.g., in occupations like dishwashing, bartending, or healthcare)
- Dermatitis
- Diabetes and HIV (increasing susceptibility)
Clinical Presentation and Diagnosis of Paronychia
Diagnosis is primarily clinical, based on the patient's history and physical examination.
History
For acute paronychia, patients report rapid onset of pain, redness, and swelling around the nail fold. Chronic cases present with recurrent tenderness and thickened nail folds. Key questions include inquiring about recent trauma, nail habits (biting, picking), recent manicures, or occupational exposures.
Physical Examination
The affected nail fold will appear red, swollen, and tender. If an abscess has formed, a fluctuant area (a collection of pus) may be palpable. In chronic paronychia, the nail folds may be retracted, thickened, and sometimes exhibit persistent discharge. The nail plate itself can become discolored or dystrophic.
Differential Diagnoses for Paronychia
It's important to differentiate paronychia from other conditions that may present with similar symptoms:
- Herpetic Whitlow: A viral infection caused by herpes simplex virus, typically presenting with grouped vesicles.
- Glomus Tumor: A benign tumor causing chronic fingertip pain and cold sensitivity.
- Subungual Melanoma: A pigmented streak under the nail, requiring specialized evaluation.
- Pyogenic Granuloma: A rapidly growing, vascular nodule that bleeds easily.
- Onychomycosis: Fungal infection of the nail plate itself.
- Nail Psoriasis: Skin condition affecting the nails, causing pitting and thickening.
- Squamous Cell Carcinoma: A rare malignant tumor affecting the nail bed.
Management of Paronychia
Treatment depends on the severity and type of paronychia.
Conservative Management
For early, uncomplicated acute paronychia, warm water or antiseptic soaks (3-4 times daily for 5-7 days) can be effective. Topical antibiotics like mupirocin or fusidic acid may be prescribed. If cellulitis extends beyond the nail fold, oral antibiotics such as flucloxacillin, cephalexin, or clindamycin may be indicated, guided by culture results if necessary.
Surgical Drainage
If an abscess is present (indicated by fluctuance or escalating pain), surgical drainage is required. This is typically performed under local anesthesia (digital block). A small incision is made parallel to the nail fold to release the pus. Care must be taken to avoid damaging the nail matrix, which can lead to deformity. If pus has tracked under the nail plate, a portion of the nail may need to be lifted or removed for adequate drainage. The area is then irrigated, and a wick may be inserted. Warm soaks and elevation are advised post-procedure.
Management of Chronic Paronychia
Treatment focuses on identifying and eliminating irritants, managing any underlying dermatitis, and addressing fungal overgrowth with topical antifungals. Short courses of topical steroids may help reduce inflammation. Surgical excision of chronically inflamed tissue is rarely necessary.
Understanding Felon
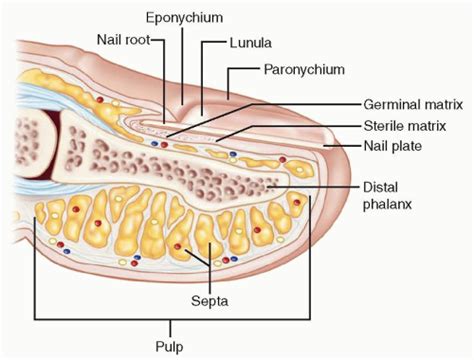
A felon is a serious infection localized within the pulp space of the fingertip. This space is divided into multiple closed compartments by fibrous septa, which can lead to rapid pressure buildup and severe pain when infected.
Causes and Pathophysiology of Felon
A felon typically results from a penetrating injury to the fingertip pulp, allowing bacteria to enter. Common causes include splinters, needle pricks, animal or human bites, or even minor cuts and abrasions.
- Penetrating Trauma: The most frequent cause, often from sharp objects.
- Untreated Paronychia: Infection can spread from the nail fold into the pulp space.
The primary pathogens are usually Staphylococcus aureus (including MRSA) and Streptococcus species. Human bites can introduce a broader range of bacteria, including anaerobes.
The rigid fibrous septa within the pulp compartments are crucial to the pathophysiology. When infection causes pus to accumulate, the pressure within these compartments rises dramatically. This increased pressure can compromise blood flow (ischemia) and venous drainage, leading to intense pain and potentially tissue necrosis if not treated promptly.
Clinical Presentation and Diagnosis of Felon
The hallmark of a felon is severe, throbbing pain in the fingertip.
History
Patients usually report a history of recent minor trauma, even if the injury seemed insignificant. They will describe intense, throbbing pain that is often worse with dependency (hanging the hand down) and is exquisitely tender to touch. Systemic symptoms like fever may be present in more severe cases.
Physical Examination
The fingertip pulp distal to the distal interphalangeal (DIP) joint will be swollen, tense, shiny, and extremely tender. Redness is common. If the infection has progressed, a fluctuant abscess may be visible or palpable. Signs of ischemia, such as altered sensation (paresthesia) or paleness, are ominous signs.
Differential Diagnoses for Felon
Similar to paronychia, other conditions can mimic a felon:
- Herpetic Whitlow: Characterized by vesicles, unlike the diffuse swelling of a felon.
- Subungual Hematoma: Discoloration under the nail following trauma.
- Glomus Tumor: Chronic, localized pain.
- Gouty Tophus or Calcinosis: Firm deposits that can mimic an abscess.
Management of Felon
Prompt treatment is essential to prevent complications.
Early Conservative Management
If there is no fluctuance and the pain is manageable, initial treatment may involve elevation, warm soaks, and oral antibiotics targeting Staphylococcus aureus (e.g., flucloxacillin, cephalexin). If MRSA is suspected, trimethoprim-sulfamethoxazole or doxycycline may be used.
Surgical Drainage
Tense, fluctuant felons require immediate surgical incision and drainage under digital block anesthesia. The key is to use an appropriate incision to release the pressure and drain the pus while minimizing damage to vital structures.
- Lateral Longitudinal Incision: This is often the preferred approach, made along the midline of the radial or ulnar side of the finger pad, avoiding the central pad where major neurovascular structures run.
- High Midline Incision: Made proximal to the DIP crease, avoiding the digital nerves and arteries. It should not extend beyond the crease.
- Avoid Transverse or "Fish-Mouth" Incisions: These carry a higher risk of damaging digital nerves and arteries and are generally reserved for complex cases.
After incision, the fibrous septa are carefully broken down bluntly, the space is irrigated thoroughly, and a wick may be placed to ensure continued drainage. The hand should be elevated post-operatively, and gentle motion can be resumed once drainage subsides.
Adjunctive Care
Appropriate oral or intravenous antibiotics are continued based on the suspected or confirmed pathogen. Patients with comorbidities like diabetes or immunosuppression require close monitoring and potentially inpatient IV therapy.

Complications of Paronychia and Felon
Delayed or inadequate management of either paronychia or felon can lead to significant morbidity and long-term consequences. Prompt recognition, appropriate antibiotic therapy, and timely surgical intervention when indicated are critical for preserving finger function.
Potential Complications
- Nail Deformity: Chronic paronychia can lead to thickened, retracted, or dystrophic nails.
- Osteomyelitis: Infection spreading to the underlying bone (distal phalanx).
- Septic Arthritis: Infection of the DIP joint.
- Flexor Tenosynovitis: Infection of the tendon sheath, a surgical emergency.
- Loss of Fingertip Sensibility: Nerve damage from infection or poorly placed surgical incisions.
- Skin Necrosis: Tissue death due to compromised blood supply, especially in untreated felons.
- Chronic Pain and Disability: Resulting from severe or untreated infections.
The fingertip pulp's unique structure, with its numerous fibrous septa, makes it particularly susceptible to intense pressure buildup during infection. A neglected felon can destroy the distal phalanx within a week due to the rapidly increasing intracompartmental pressure, which can exceed 100 mmHg and cut off arterial inflow.
Paronychia - Everything You Need To Know - Dr. Nabil Ebraheim
tags: #paronychia #and #felon