Recognizing and differentiating childhood rashes is crucial for accurate diagnosis, as appearance alone can be misleading. A comprehensive approach that considers the rash's characteristics, clinical course, and associated symptoms is essential.
Key Considerations for Diagnosing Pediatric Rashes
When evaluating a rash in a child, several factors come into play:
- Appearance and Location: The visual presentation and where the rash is situated on the body provide important clues.
- Clinical Course: How the rash has evolved over time, including its onset and progression, is significant.
- Associated Symptoms: The presence or absence of symptoms like itching (pruritus) or fever can help narrow down the possibilities.
Rashes Associated with Fever
A fever is often present with certain childhood rashes, including:
- Roseola: Characterized by a rash appearing after the resolution of a high fever.
- Erythema Infectiosum (Fifth Disease): Also known for a fever that precedes the rash.
- Scarlet Fever: Typically accompanied by fever and sore throat before the rash develops.
Rashes Associated with Pruritus (Itching)
Itching can be a prominent symptom in several types of rashes:
- Atopic dermatitis
- Pityriasis rosea
- Erythema infectiosum
- Molluscum contagiosum
- Tinea infection
Common Types of Pediatric Rashes and Their Characteristics
Differentiating between various types of rashes can be challenging. Understanding the key features of common pediatric rashes is vital for primary care physicians, who manage a significant percentage of these cases.
Viral Infections and Their Rashes

Roseola (Exanthema Subitum or Sixth Disease)
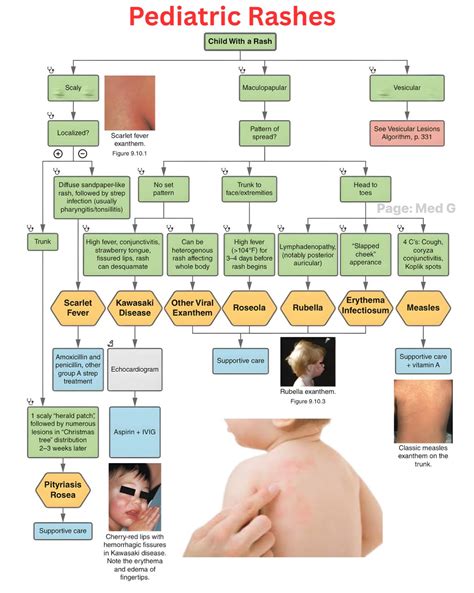
Roseola, most commonly caused by human herpesvirus 6, typically affects infants and children younger than three years. It is characterized by the abrupt onset of a high fever lasting one to five days. During this febrile period, children usually appear well with minimal clinical signs, possibly including a mild cough, rhinorrhea, or diarrhea. Once the fever resolves, an erythematous macular to maculopapular rash typically emerges, starting on the trunk and spreading peripherally. This rash can resemble rubeola (measles), but in roseola, the rash appears after the fever breaks, whereas measles rash usually begins on the face.
Erythema Infectiosum (Fifth Disease)
Erythema infectiosum, caused by parvovirus B19, is a common childhood infection. It begins with a prodrome of low-grade fever, malaise, sore throat, headache, and nausea. This is followed several days later by a characteristic erythematous “slapped cheek” facial rash. After two to four days, the facial rash fades, and a pink, lacy, reticular rash may develop on the extremities. While patients are no longer infectious once the rash appears, the rash can reappear with sun exposure, heat, or stress. Arthralgias are more common in older children and adults.
Molluscum Contagiosum
Molluscum contagiosum is a highly contagious viral infection caused by a poxvirus, predominantly affecting children aged two to 11 years. The lesions are typically flesh-colored or pearly white, small papules with central umbilication. While the oral mucosa is rarely involved, lesions can appear on the genital region and conjunctiva. Children may have 10 to 20 lesions, but some can have hundreds. The condition is usually self-limited and resolves without intervention, though treatment options exist for cosmetic concerns.
Chickenpox (Varicella)
Chickenpox, now less common due to vaccination, presents with itchy, blister-like bumps that appear in waves. The rash often starts on the scalp, face, or torso and spreads throughout the body, progressing from red bumps to fluid-filled blisters that eventually form dry crusts or scabs.
Measles (Rubeola)
Measles is a highly contagious viral infection that begins with cold-like symptoms and is followed by a spreading rash. The rash typically starts on the face, often behind the ears, and moves downward. Koplik spots may appear in the mouth. Children with measles are usually more ill-appearing than those with roseola.
Rubella (German Measles)
Rubella causes a pinkish rash that usually starts on the face and spreads downward. It can resemble measles but is caused by a different virus. Vaccination helps prevent rubella.
Hand, Foot, and Mouth Disease
This common illness causes tiny blisters or spots on the hands, feet, and sometimes the legs or diaper area, along with painful mouth sores.
Bacterial Infections and Their Rashes
Scarlet Fever
Scarlet fever, caused by certain strains of group A beta-hemolytic streptococci, is diagnosed in a percentage of children presenting with streptococcal tonsillopharyngitis. It typically presents with fever and sore throat one to two days before a rash develops on the upper trunk, spreading throughout the body while sparing the palms and soles. The rash is characterized by confluent, erythematous, blanching, fine macules resembling a sunburn, with sandpaper-like papules. In skinfolds, erythematous, nonblanching linear eruptions (Pastia lines) may appear. Petechiae on the palate and a “strawberry tongue” are also characteristic. Penicillin is the primary treatment.
Impetigo
Impetigo is a superficial bacterial infection of the epidermis. It can be primary, occurring when bacteria enter breaks in the skin, or secondary, developing at the site of an existing dermatosis. There are bullous and nonbullous forms. The nonbullous form, common in preschool- and school-aged children, typically begins as vesicles or pustules that form a thick, yellow crust, often spreading rapidly through autoinoculation. The face and extremities are most commonly affected.
Fungal Infections and Their Rashes
Tinea (Ringworm)
Tinea is a common fungal skin infection in children affecting various body parts, including the scalp (tinea capitis), body (tinea corporis), groin (tinea cruris), feet (tinea pedis), hands (tinea manus), or nails (tinea unguium). Tinea capitis is characterized by scaling, circumscribed alopecia, and broken hair follicles, often with posterior cervical lymphadenopathy. Tinea corporis typically presents as an erythematous annular patch or plaque with a raised border and central clearing, often with scaling along the border, commonly referred to as ringworm.
Dermatitis and Other Inflammatory Conditions
Atopic Dermatitis (Eczema)
Atopic dermatitis is a chronic, relapsing inflammatory skin condition that can present with various skin changes. It is characterized by dryness, itching, and inflammation. The distribution of lesions varies with age; infants and younger children often have lesions on extensor surfaces, cheeks, and scalp, while older children and adults may have patches and plaques on flexor surfaces. In severe cases, thickened, lichenified plaques may be present. Children with atopic dermatitis are at risk of secondary skin infections.
Contact Dermatitis
This type of rash occurs when the skin comes into contact with an irritating or allergenic substance, leading to redness, itching, or small bumps.
Diaper Rash
A common rash in infants, typically appearing on the buttocks, thighs, or genital area due to moisture, friction, or irritation from diapers. It can sometimes be complicated by a yeast infection.
Cradle Cap (Infant Seborrheic Dermatitis)
A harmless condition affecting a baby's scalp, characterized by flaky, sometimes greasy patches.
Hives (Urticaria)
Red, itchy bumps that can appear on the body, face, and hands, often as a reaction to an allergen. They may come and go and can persist for varying durations.
Baby Acne
Breakouts on a newborn's face and chest that usually resolve on their own within the first few months of life.
Identifying Pediatric Rashes at Home
While online photos can be a starting point, a thorough assessment of symptoms and changes over time is crucial for understanding a child's rash. Key factors to observe include:
- Itching: Severity from mild to intense.
- Fever or Cold Symptoms: Viral rashes often follow an illness.
- Color: Bright red, pink, purplish, blotchy, or streaked.
- Shape: Rings, clusters, patches, or lines.
- Texture: Raised, sandpaper-like, smooth, or scaly.
- Speed of Spread: Changes occurring over hours versus days can help narrow down the cause.
Prevention and Home Care for Mild Rashes
While not all rashes can be prevented, several everyday practices can help reduce the risk of skin irritations and infections:
- Avoid Triggers: Steer clear of known allergens or products that irritate the skin.
- Good Hygiene: Encourage frequent handwashing, especially after outdoor play.
- Avoid Picking: Advise against picking or scratching at cuts, scrapes, or healing skin.
- Cough/Sneeze Etiquette: Cover coughs and sneezes with the elbow to prevent germ spread.
- Limit Exposure: Maintain distance from individuals with contagious illnesses.
- Vaccinations: Ensure timely vaccinations to prevent infections like chickenpox, measles, and rubella.
When to Seek Urgent Medical Care for a Rash
Immediate medical attention is necessary if a rash is accompanied by any of the following symptoms:
- Increasing pain, redness, or unusual discoloration at the rash site.
- Tightness, swelling, or itching in the throat.
- Difficulty breathing.
- Swelling of the face, lips, or limbs.
- Fever of 100.4°F (38°C) or higher.
- Confusion or dizziness.
- Severe headache or neck pain.
- Persistent vomiting or diarrhea.
Medical care is also recommended if a rash occurs with systemic signs such as:
- Joint pain or swelling.
- Sore throat.
- Red streaks or tender areas near the rash.
- A recent tick bite or animal bite.
Measles: Rashes in the paediatric emergency department.
Prompt evaluation by a healthcare provider is crucial in these situations.