Topical skin adhesives, particularly 2-octyl cyanoacrylate, have emerged as a valuable tool in wound closure, offering a convenient and effective alternative to traditional methods like sutures and staples. These sterile, liquid adhesives are designed to hold wound edges together, forming a flexible film that naturally sloughs off the skin within 5 to 10 days.
Indications and Applications
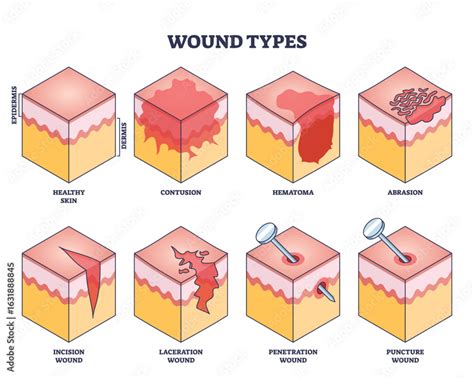
The primary indication for 2-octyl cyanoacrylate includes easily approximated surgical incision wounds and properly cleaned lacerations from trauma. These applications are most suitable for dry areas with minimal friction. Initially approved by the U.S. Food and Drug Administration (FDA) in 1998 as an alternative to 5-0 or smaller sutures, staples, or adhesive strips, its use has expanded.
Additionally, 2-octyl cyanoacrylate is approved for use in conjunction with subcuticular sutures for deeper or higher tension wounds. While initial FDA labeling cautioned against its use in high-tension areas without immobilization, subsequent research has shown comparable results in wound dehiscence and scar formation between suture repair and 2-octyl cyanoacrylate closure on properly immobilized high-tension areas.
Emerging applications, though not extensively studied for initial FDA approval, include mucosal repair. Case reports highlight successful repair of tongue lacerations, and blinded comparisons have demonstrated equivalent cosmetic outcomes to sutures in cleft lip repair regarding wound dehiscence and scar formation.
Mechanism of Action
The efficacy of 2-octyl cyanoacrylate lies in its polymerization process. Before application, the adhesive exists as monomers. Upon contact with anions from skin moisture or wound exudate, these monomers undergo a rapid, exothermic polymerization reaction. This process binds the adhesive to the most superficial epithelium, creating a cyanoacrylate bridge that forms a watertight barrier over the approximated wound edges. This barrier facilitates uninterrupted wound healing.
Beyond its physical barrier function, 2-octyl cyanoacrylate exhibits intrinsic antimicrobial activity against both gram-positive (including methicillin-resistant Staphylococcus aureus) and non-pseudomonas gram-negative bacteria. A hypothesized mechanism for this antimicrobial effect involves the destabilization of bacterial cell capsules through electromagnetic interactions between the negatively charged adhesive and the positively charged bacterial capsule.
Administration and Application Techniques
2-octyl cyanoacrylate is available in various forms, including a gel, a high-viscosity option, a mini-applicator, and a combination mesh/glue system. The high-viscosity formulation is marketed to complement deep dermal sutures and reduce unintended migration during application. The mesh/glue system involves serial administration of self-adhering mesh followed by the adhesive.
Proper application requires several key steps:
- Administration of local anesthesia.
- Thorough wound irrigation.
- Adherence to antiseptic techniques.
- Having petroleum jelly readily available for adhesive removal if necessary.
- Manual approximation and slight eversion of wound edges.
- Application of three layers of adhesive, with maximal bonding strength achieved within 2.5 minutes.
Special precautions are necessary for facial applications to prevent the gel from contacting or entering the eyes, ears, or nose. Care must also be taken to avoid inadvertent adhesion of the practitioner's hands or gloves to the patient's skin.
Adverse Effects and Contraindications
While generally safe, topical skin adhesives can lead to adverse effects. Mild swelling, redness, and pain around the wound site are common and typically resolve as the wound heals. Increased swelling, redness, or pain, or a sensation of warmth at the application site, may indicate a problem and warrant physician contact. Prolonged exposure to sunlight or tanning lamps should be avoided while the adhesive film is in place.
The risk of wound infection with 2-octyl cyanoacrylate is statistically similar to that of traditional suture repair. In rare instances, contact allergic dermatitis may occur during or after treatment, with reactions usually resolving within a few days, though occasionally persisting for months.
Explicit contraindications for using 2-octyl cyanoacrylate include:
- Gangrenous, actively infected, or decubitus injuries.
- Patients with a known hypersensitivity to cyanoacrylate or formaldehyde.
Several conditions are considered inappropriate for 2-octyl cyanoacrylate use due to a lack of study or increased risk:
- Wounds in high moisture or friction areas (e.g., axilla, other intertriginous areas).
- Animal or human bites.
- Stab or puncture wounds.
- Vermillion surface wounds.
- Patients with burst stellate lacerations.
- Patients with peripheral vascular disease, clotting disorders, insulin-dependent diabetes, or a personal/family history of keloid formation or hypertrophy.
It is crucial to avoid applying liquid or ointment medications or any other product to the wound while the adhesive film is in place, as this may loosen the film prematurely. Patients should also avoid soaking, scrubbing, swimming, and periods of heavy perspiration until the adhesive has naturally fallen off. After showering or bathing, the wound should be gently blotted dry.
Monitoring and Follow-up
In most cases, no specific follow-up is required after the application of 2-octyl cyanoacrylate, as the epithelial layer and adhesive will spontaneously slough off within 5 to 10 days. Patients should be instructed on proper wound hygiene, avoiding excessive scrubbing or picking that could increase dehiscence rates.
Although 2-octyl cyanoacrylate acts as a waterproof barrier, prolonged exposure to water should be avoided to prevent premature erosion of the adhesive. As mentioned, no topical antibiotics or other medications should be applied directly onto the adhesive. Patients should remain vigilant for signs of wound dehiscence or infection, such as erythema, edema, or purulent discharge, and contact their physician if these occur.
Toxicity and Chemical Considerations
Earlier precursors of 2-octyl cyanoacrylate, such as ethyl-2 cyanoacrylate, had similar bonding capabilities but degraded into cyanoacetate and formaldehyde, leading to inflammatory reactions. 2-octyl cyanoacrylate addresses this by using longer-chain products that undergo slower release and safer natural excretion. However, individuals with hypersensitivity to cyanoacrylate or formaldehyde can still develop contact dermatitis.
Enhancing Healthcare Team Outcomes
The effective and efficient application of 2-octyl cyanoacrylate is optimized through an interprofessional approach within the healthcare team, particularly in pediatric care. Collaboration among nursing staff, physicians, and patient care technicians is essential for tasks such as wound irrigation, adhesive application, and patient stabilization. Specialized wound-care nurses play a vital role in ensuring proper wound management, educating ancillary staff and patients on follow-up care, and promptly reporting any emerging issues to the managing physician. This coordinated effort among clinicians, nurses, and support staff is critical for successful outcomes when utilizing topical skin adhesives.