Vitamin D, often referred to as the "sunshine" vitamin, has garnered significant attention due to the prevalent deficiency observed worldwide. Initially recognized for its critical role in bone health, recent research has unveiled its importance across various bodily systems, including the brain, heart, muscles, immune system, and notably, skin health. This broad bio-functionality stems from its distinct biological activity in nearly every human tissue, making its deficiency a potential contributor to numerous diseases, particularly dermatological conditions.
The synthesis of vitamin D involves diverse methodologies, and while plasma levels are influenced by multiple factors, its role in skin health has become a focal point. Studies have demonstrated vitamin D's efficacy against skin diseases such as psoriasis, atopic dermatitis, vitiligo, acne, and rosacea. This review critically examines the relationship between vitamin D and skin health, with a particular emphasis on its potential applications and benefits in cosmetic and skincare products.
Historical Context and Discovery of Vitamin D
The history of understanding vitamin D's significance dates back to the 17th century with the outbreak of rickets, a disease profoundly impacting global populations. Daniel Whistler first described "Rickets" in 1645, recognizing it as a hallmark of vitamin D deficiency. However, it took nearly three centuries for scientists to fully appreciate vitamin D's potential as a protective, preventative, and therapeutic agent.
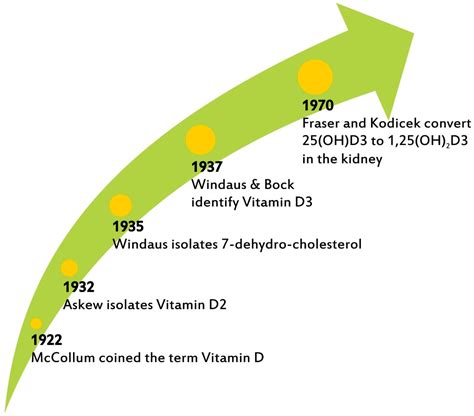
In 1919, Kurt Huldschinsky proposed that ultraviolet B (UVB) rays could effectively treat rickets. Concurrently, Sir Edward Mellanby (1920) identified dietary vitamin D deficiency as a contributing factor, particularly the lack of a vital component found in cod liver oil. Building on this, E. V. McCollum, through extensive animal studies, succeeded in distinguishing the biological activities of fat-soluble vitamins A and D, subsequently naming the latter "vitamin D" in 1922.
Chemical Characterization and Early Research
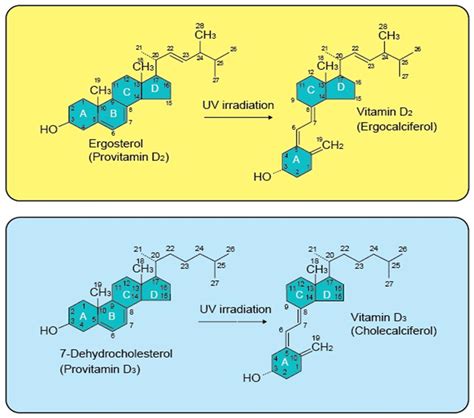
Despite its recognized importance, the precise chemical structure of vitamin D remained elusive for some time. In 1937, Windaus and Bock collaborated to establish the chemical characterization of vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol). Vitamin D2 was synthesized by UV irradiation of ergosterol (found in plants and yeast), while vitamin D3 was produced via UV irradiation of 7-dehydrocholesterol. Notably, vitamin D3 was identified as the active antirachitic constituent in cod liver oil.
These discoveries classified vitamin D as a steroid, specifically a bioactive secosteroid. Further experimental proof by Nicolayson in 1937 demonstrated vitamin D's essentiality for calcium absorption. Sixteen years later, he also confirmed that a low-calcium diet could enhance calcium absorption.
Unveiling the Active Forms and Receptors
The isolation of 25-hydroxy vitamin D3 (25(OH)D3) by DeLuca in 1968, followed by the discovery of the vitamin D receptor (VDR) by Mark Haussler in 1969, paved the way for the identification and characterization of 1α,25-dihydroxy-vitamin D3 (1α,25(OH)2D3), also known as calcitriol, by Hector DeLuca and Anthony Norman in 1971.
Validated research indicated that 1α,25(OH)2D3 interacts with the VDR to modulate gene transcription in various cell types. This was further supported by the discovery that human and other genomes enable gene regulation by 1α,25(OH)2D3, impacting genes across the entire genome. While DeLuca confirmed the skin's role in vitamin D synthesis in 1978, other researchers during this period began associating vitamin D with multiple disease risks, a correlation explored in numerous preclinical and clinical studies.
Evolution of Vitamin D Research Eras
Vitamin D research has progressed through distinct phases:
- The Transcription Era (1971-2000): Focused on the molecular and cellular mechanisms of vitamin D.
- The Association Era (1980-2010): Examined the links between vitamin D levels and various health outcomes.
- The Genomics Era (2000-Present): Emphasizes the exploration of genetic variations influencing vitamin D metabolism.
Clinical trials historically centered on bone health and the prevention of conditions like osteoporosis and rickets. More recently, the focus has shifted to investigating vitamin D's non-skeletal effects, including its role in modulating immune function, reducing inflammation, and managing chronic diseases such as cancer and cardiovascular disorders.
Chemical Structure, Sources, and Functions of Vitamin D
Vitamin D is a naturally occurring, fat-soluble photoproduct found in plants, human skin, and animal skin. Vitamin D2 is primarily derived from plants, while vitamin D3 is mainly found in animal and human skin. Both forms exhibit similar effects and potency and undergo comparable metabolic processes.
Types and Synthesis of Vitamin D
Vitamin D is synthesized when fungi, plants, animal skin, and human skin are exposed to UVB radiation. While other forms like D1, D4, and D5 exist, they hold minor significance for humans. Chemically, vitamin D shares a structure with cholesterol, featuring four rings (A, B, C, and D), with a broken B ring distinguishing it from cholesterol.
The primary forms are:
- Vitamin D2 (Ergocalciferol): Derived from ergosterol, found in plants and yeast, synthesized by UV irradiation of ergosterol.
- Vitamin D3 (Cholecalciferol): Derived from 7-dehydrocholesterol in animal and human skin, synthesized by UV irradiation of 7-dehydrocholesterol.
Minor structural differences, such as an additional double bond and a methyl group at carbon 24 in vitamin D2, influence their stability and metabolism.
Natural Sources and Absorption
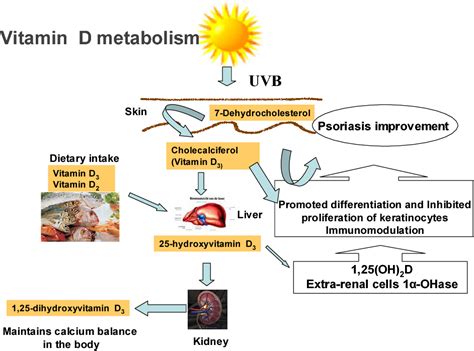
Sunlight is the most significant natural source of vitamin D. UVB rays convert 7-dehydrocholesterol in the skin into provitamin D3, which then transforms into vitamin D3. Factors like latitude, season, time of day, skin pigmentation, age, and sunscreen use can affect the skin's ability to produce vitamin D3.
Dietary sources include fatty fish (salmon, mackerel, sardines), cod liver oil, egg yolks, and fortified dairy products. For individuals with limited sun exposure or specific metabolic conditions, vitamin D supplements are crucial.
Metabolism and Active Form
Upon absorption, vitamin D3 travels to the liver, where enzymes convert it to 25(OH)D3. Subsequently, this compound is transformed into the active form, 1α,25(OH)2D3 (calcitriol), primarily in the kidneys. Calcitriol acts as a hormone, regulating numerous biochemical cascades and homeostasis systems.
Vitamin D in Skincare Products
Vitamin D's integration into skincare products leverages its diverse beneficial properties. While topical application offers localized benefits, it's important to distinguish between cosmetic formulations and medical preparations.
Cosmetic Applications of Vitamin D
Many cells, particularly skin cells, possess the capacity to produce vitamin D and its active form, highlighting its localized role. Vitamin D is classified as a fat-soluble prohormone, with its active form functioning as a hormone. The active complex, 1α,25(OH)2D3, is a significant regulator of biochemical processes and homeostasis.
The discovery of vitamin D's remarkable properties has spurred the development of various skincare products, cosmetic formulations, and topical analogs. Its anti-inflammatory, anti-melanoma, anti-cancer, anti-UV, anti-aging, and antioxidant properties have been harnessed for conditions such as psoriasis, atopic dermatitis, vitiligo, acne, and rosacea.
Topical Vitamin D Analogues for Medical Conditions
Vitamin D cream, in a medical context, refers to prescription topical preparations containing synthetic vitamin D analogues like calcipotriol, tacalcitol, or calcitriol. These are not nutritional supplements but regulated medicines primarily used to treat psoriasis and other dermatological conditions. They function by slowing excessive skin cell proliferation and promoting normal cell maturation.
In the UK, these prescription creams are regulated by the MHRA and recommended by NICE as a first-line treatment for mild to moderate plaque psoriasis, often in combination with corticosteroids.
Mechanism of Action of Topical Vitamin D Analogues
When applied topically, vitamin D analogues bind to vitamin D receptors (VDR) in skin cells, particularly keratinocytes. This interaction modulates gene expression and cellular behavior. The primary mechanism involves reducing the rapid multiplication of skin cells and promoting their normal differentiation and maturation. Additionally, these preparations exhibit mild anti-inflammatory effects by modulating immune cell activity in the skin, reducing pro-inflammatory cytokines and the infiltration of inflammatory cells.
It is crucial to differentiate between medical-grade topical vitamin D analogues and cosmetic products containing vitamin D or its precursors. The former are regulated as medicines and possess therapeutic potency, unlike the latter.
Medical Uses of Vitamin D Cream
The primary licensed indication for topical vitamin D cream in the UK is psoriasis, a chronic inflammatory skin condition characterized by red, scaly patches. Calcipotriol is particularly effective for plaque psoriasis, which constitutes the majority of psoriasis cases.
Psoriasis Treatment
For psoriasis on the trunk and limbs, NICE recommends either a vitamin D analogue applied once or twice daily for up to 8 weeks, or a potent corticosteroid applied once daily in combination with a vitamin D analogue once daily for up to 4 weeks. Combination products containing calcipotriol and betamethasone dipropionate are widely prescribed, offering rapid anti-inflammatory relief from the corticosteroid and addressing abnormal cell proliferation with the vitamin D analogue.
While some patients see improvements within two weeks, optimal results typically require 6-8 weeks of consistent application. Regular review by a healthcare professional is recommended to assess treatment response and adjust therapy. Psoriasis is a chronic condition requiring ongoing management as part of a broader treatment strategy.
Other Hyperproliferative Skin Conditions
Topical vitamin D creams may occasionally be used off-label for other hyperproliferative skin conditions, though evidence for such uses is limited. Treatment duration and expected outcomes can vary significantly among individuals.
Application and Safety of Topical Vitamin D Cream
Proper application techniques are essential for maximizing efficacy and minimizing potential adverse effects when using topical vitamin D creams.
Safe Application Practices
Vitamin D cream should be applied thinly and evenly to affected areas only, avoiding healthy surrounding skin. The typical dosage frequency is once or twice daily, as per prescriber instructions. Ensure the skin is clean and dry before application. Thoroughly wash hands before and after application, unless treating the hands themselves.
Use only the prescribed amount; overapplication does not enhance results and may increase the risk of side effects. Exercise caution when applying to facial or flexural areas (skin folds), as these regions are more sensitive. Some vitamin D preparations are not licensed for facial or flexural use due to an increased risk of irritation.
Precautions and Contraindications
Maximum weekly dose limits apply to prevent excessive vitamin D absorption, which could affect calcium metabolism. Avoid application to eyes, mucous membranes, or broken/infected skin. Limit excessive exposure to natural or artificial UV light.
Inform your prescriber if you are pregnant, planning pregnancy, or breastfeeding, as safety data are limited. Topical salicylic acid should not be used on the same treatment area as it may inactivate some vitamin D analogues. Separate application from emollients by approximately 30 minutes.
Store vitamin D creams according to package instructions, typically at room temperature away from direct heat and light. Some formulations may be flammable. If a dose is missed, apply it as soon as remembered, unless it is close to the next scheduled dose.
Potential Side Effects
Topical vitamin D creams are generally well-tolerated, but side effects can occur. The most common adverse effects are local skin reactions at the application site, including mild irritation, itching, redness, burning, or dryness. Less commonly, patients may experience dermatitis, skin discoloration, or a paradoxical worsening of psoriasis symptoms.
Systemic side effects are rare with appropriate topical use due to limited absorption through intact skin. However, excessive application over large body surface areas or with occlusive dressings could theoretically lead to hypercalcemia (elevated blood calcium) or hypercalciuria (elevated urinary calcium). Known disorders of calcium metabolism or hypercalcemia are contraindications for use.
Patients should seek medical attention for signs of allergic reaction, severe skin irritation, or symptoms suggesting calcium disturbance. Regular monitoring of calcium levels is not typically required for localized treatment but may be considered for extensive disease requiring large quantities of cream.
Alternatives to Topical Vitamin D Treatments
Various alternative treatments exist for conditions managed with topical vitamin D, with the choice depending on disease severity, location, patient preference, and treatment response.
Other Topical Treatments
- Topical Corticosteroids: A cornerstone of psoriasis management, often used alongside or as alternatives to vitamin D analogues.
- Emollients and Moisturisers: Essential for managing dry, scaly skin conditions, reducing scaling, improving skin barrier function, and enhancing comfort.
- Coal Tar Preparations: Traditional treatments with anti-inflammatory and antiproliferative properties, available in various formulations but sometimes considered less cosmetically acceptable due to odor and staining.
Phototherapy and Systemic Therapies
- Phototherapy: Offers an effective alternative for patients unresponsive to or intolerant of topical treatments. Narrowband UVB is typically used first-line, with PUVA reserved for specific cases, administered in hospital dermatology departments.
- Systemic Therapies: For severe, extensive, or treatment-resistant disease, systemic treatments may be necessary. These include conventional immunosuppressants (methotrexate, ciclosporin), oral retinoids (acitretin), or biologic agents. These require specialist dermatology input and careful risk-benefit assessment.
NICE recommends referral for specialist assessment if psoriasis is severe, significantly impacts well-being, or does not respond to topical therapy. Urgent referral is necessary for unstable erythrodermic or generalized pustular psoriasis.
Frequently Asked Questions
Is vitamin D cream available over the counter in the UK?
No, vitamin D cream containing therapeutic analogues like calcipotriol is available only on prescription in the UK. These are regulated medicines licensed for specific dermatological conditions, not cosmetic products or nutritional supplements.
How long does vitamin D cream take to work for psoriasis?
Some patients notice improvement within two weeks, though optimal results typically require 6-8 weeks of consistent application. Regular review by a GP or dermatologist is recommended to assess treatment response.
Can I use vitamin D cream on my face?
Most vitamin D cream preparations, particularly calcipotriol, are not licensed for facial use due to increased irritation risk on thinner, more sensitive facial skin. Vitamin D derivatives come in various formulations, including gel, ointment, lotion, and scalp solutions, acting by normalizing skin cell growth and preventing excessive proliferation seen in psoriasis.
What are Vitamin D treatments?
Topical vitamin D treatments are often among the first prescribed for psoriasis. They can be in ointment, lotion, gel, or foam formulations. With few exceptions, they are available only by prescription. Some pharmacies may sell Dovonex ointment over the counter at a higher cost. These treatments slow down skin cell production and have an anti-inflammatory effect, improving psoriasis symptoms. They are distinct from oral vitamin D supplements.
When should vitamin D treatments be used?
Topical vitamin D treatments can be used alone or in combination with topical steroids. A review appointment is recommended four weeks after starting any new topical treatment to assess results and provide assistance. Like all topical treatments, it may take several weeks for vitamin D treatment to become fully effective.