Eczema, also known as dermatitis, is a group of chronic skin conditions characterized by inflamed, dry, itchy, red, and irritated skin. It is not contagious and can manifest with rashes, blisters, scaly patches, weeping skin, and infections. The affected skin may also change color, appearing gray, purple, or deep brown on darker skin tones, and red or pink on lighter skin tones. Over time, the rash can become thick and hard.
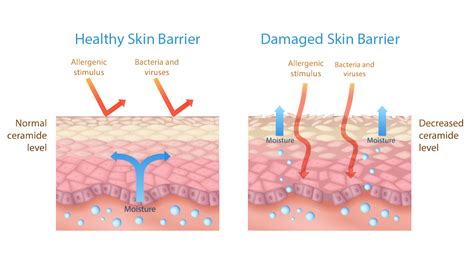
Eczema significantly weakens the skin barrier, which is crucial for retaining moisture and protecting the body from external irritants, infections, and allergens. This compromised barrier function is a central hypothesis in understanding the development of eczema.
The Structure of Healthy Skin
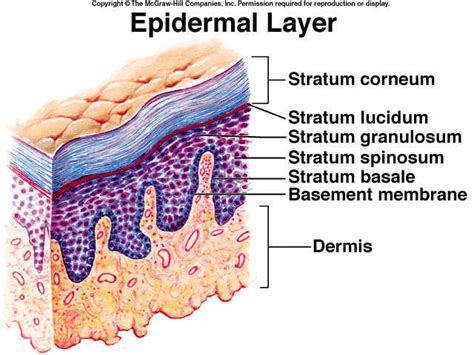
The skin is composed of three primary layers: the superficial epidermis, the deeper dermis, and the innermost subcutis. The epidermis itself is further divided into several sub-layers. In thick skin, found on the palms of the hands and soles of the feet, the epidermis consists of five layers: the stratum basale, stratum spinosum, stratum granulosum, stratum lucidum, and the outermost stratum corneum. In thin skin, covering the rest of the body, the stratum lucidum is absent, resulting in four layers.
Key Epidermal Layers and Their Functions:
- Stratum corneum: This is the most superficial layer, composed of dead cells that are tightly packed and rich in keratin. This layer provides a protective coating against environmental pathogens and contributes to water resistance.
- Stratum granulosum: Cells in this layer release granules that form a lipid-rich substance, contributing to the skin's barrier function and water retention.
- Stratum spinosum: Cells in this layer are tightly bound together, forming strong intercellular connections.
- Stratum basale: This is the deepest layer of the epidermis where new skin cells are produced.
The dermis, located beneath the epidermis, has two main layers: the papillary layer and the reticular layer. The papillary layer, composed of loose connective tissue, anchors the epidermis and contains capillaries that nourish the epidermis and remove waste products. The reticular layer, the deepest part of the dermis, is made of densely interwoven connective tissue fibers that surround blood vessels, nerves, hair follicles, and glands. These fibers extend into the subcutaneous tissue and the papillary layer.
Accessory structures of the skin, such as hair, nails, and glands, also play a role in protection. Sebaceous glands, for example, produce sebum, an oily lipid that lubricates the skin and hair. Some sebaceous follicles are large and communicate directly with the epidermis, particularly on the face, back, and chest.
Understanding Eczema (Dermatitis)
Eczema is a chronic, non-infectious inflammatory skin condition. While it can appear as a single episode, it often recurs. The primary symptom is intense itching, which can significantly impact a person's quality of life, affecting concentration and sleep. Rashes associated with eczema are not contagious. Symptoms can vary widely, with affected skin becoming dry, scaly, red, swollen, or even weeping and crusty. In more severe cases, the skin may thicken and crack.
The skin barrier in individuals with eczema is compromised. This disruption allows irritants, germs, and allergens to penetrate the skin more easily. Research indicates that a deficiency in the protein filaggrin, crucial for the formation of the outer skin layer, is a common genetic factor in eczema. This deficiency affects the skin's lipid balance, leading to increased moisture loss.
Eczema Affects Skin Layers
In individuals with eczema, the stratum corneum, the outermost layer of the epidermis, does not provide adequate protection due to inflammation. This compromised barrier allows irritants and allergens to enter the skin more readily. Furthermore, studies have identified a defect in a second skin barrier structure: the tight junctions. These are cell-to-cell connections that regulate the permeability of the skin. A specific protein, claudin-1, which determines the strength and permeability of these tight junctions, is significantly reduced in the skin of eczema patients compared to healthy individuals or those with psoriasis.
The weakened skin barrier leads to increased transepidermal water loss (TEWL), meaning the skin loses moisture more rapidly. This dryness exacerbates itching and makes the skin more susceptible to infection and irritation.
Types of Eczema
There are several types of eczema, many of which are related to allergies:
- Atopic dermatitis: The most common form, often triggered by allergens, irritants, chemicals, temperature changes, and emotions. It causes dry, itchy skin and rashes.
- Contact dermatitis: An allergic reaction caused by direct contact with irritants or allergens like nickel, poison ivy, or latex.
- Dyshidrotic eczema: Characterized by tiny, itchy blisters on the hands and feet, which can be painful and cause a burning sensation.
- Hand eczema: Affects the skin on the hands, often seen in individuals frequently exposed to water or chemicals.
- Neurodermatitis: Begins with an itchy patch of skin that intensifies with scratching, often worse at night.
- Nummular eczema: Presents as small, raised, round, itchy spots, often triggered by skin injury, infection, or stress.
- Seborrheic dermatitis: Typically affects the scalp.
- Stasis dermatitis: Occurs in individuals with poor blood circulation, commonly on the ankles, leading to skin discoloration.
Causes and Triggers of Eczema
Eczema is believed to result from a complex interplay of genetic predisposition and environmental factors. While the exact cause is unknown, several factors increase the likelihood of developing eczema:
- Genetic predisposition: Eczema often runs in families, and a deficiency in filaggrin is a significant genetic link.
- Sensitive immune system: Individuals with asthma, hay fever, and other allergies are more prone to eczema. The immune system in eczema patients may have an enhanced response to stimuli.
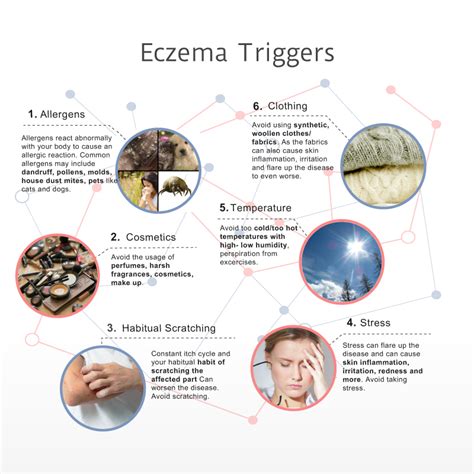
- Environmental factors: Various substances can trigger eczema flare-ups, including:
- Allergens: dust mites, pet dander, certain foods, pollen, latex.
- Irritants: soaps, detergents, lotions, household cleaners, fragrances, dyes, chemicals like formaldehyde.
- Metals: nickel (found in jewelry, belt buckles, etc.).
- Stress and emotions.
- Temperature and humidity changes (heat, cold, dry weather).
- Infections, such as Staphylococcus aureus (staph).
Factors like pollution and increased hygiene standards are also thought to contribute to the rising prevalence of eczema.
Diagnosis of Eczema
Doctors diagnose eczema through a physical examination and a review of the patient's medical and family history. They will inquire about symptoms, their onset, and potential triggers. The location of the rash can also provide clues; infants often develop rashes on their face and limbs, while older children and adults may have them in skin folds and on hands or eyelids.
Additional diagnostic tests may include:
- Allergy testing: Skin prick tests or blood tests (IgE tests) can identify specific allergies.
- Patch testing: Used to diagnose contact dermatitis, this involves applying small amounts of suspected allergens to the skin under patches for a period to observe for a reaction.
Routine lab work is generally not recommended for diagnosing eczema.
Symptoms of Eczema
The symptoms of eczema are diverse and can change over time. Common signs include:
- Dry, scaly, or rough skin patches.
- Intense itching.
- Inflamed or swollen skin.
- Oozing or crusty skin.
- Discolored skin (red on lighter skin, ashen, purple, or dark brown on darker skin).
- Skin thickening over time.
In babies, eczema commonly appears on the cheeks, scalp, and the outer surfaces of arms and legs. In older children and adults, it often affects the creases of the elbows and knees, the neck, wrists, and ankles. While most children outgrow eczema, it can persist into adulthood or reoccur, often affecting the hands.
Treatments and Management
There is no cure for eczema, but its symptoms can be effectively managed through a combination of treatments and lifestyle adjustments:
1. Avoiding Triggers:
Identifying and avoiding personal eczema triggers is a primary management strategy. This can include allergens, irritants, certain fabrics, and extreme temperatures.
2. Skincare Routine:
- Moisturization: Regularly applying emollients (lotions, creams, ointments, petroleum jelly) helps to hydrate the skin and reinforce the skin barrier.
- Bathing: Short, lukewarm baths or showers are recommended. Using mild, unscented cleansers instead of harsh soaps is important. Patting the skin dry gently after bathing is crucial.
- Bleach Baths: For individuals prone to skin infections, doctors may recommend diluted bleach baths (adding a small amount of bleach to bathwater) 2-3 times a week to reduce bacteria on the skin.
- Wet Wrapping: In severe cases, after moisturizing, damp gauze or clothing is wrapped around affected areas to enhance hydration and rehydration.
3. Medications:
- Over-the-counter and prescription creams: Hydrocortisone creams reduce inflammation. Stronger corticosteroid creams and topical calcineurin inhibitors (TCIs) are available by prescription.
- Biologics: Medications like Dupixent® and Adbry® target specific inflammatory pathways.
- Antihistamines: May help with associated allergies but do not typically alleviate eczema itching.
- Antibiotics: Used to treat secondary bacterial skin infections.
- Phototherapy: Treatment using ultraviolet (UV) light under medical supervision.
It is essential to consult a doctor to develop a personalized treatment and management plan.
Understanding Eczema: The Itch-Rash Cycle & The "Soak & Seal" Protocol
Managing eczema can be challenging, but with consistent skincare, trigger avoidance, and appropriate medical treatment, individuals can significantly improve their quality of life, reduce pain and itching, prevent infections, and control flare-ups.