Understanding the Connection Between the Nervous System and Psoriasis
Prior research has demonstrated that neurotransmitters may play a role in the pathogenesis of numerous cutaneous conditions, including psoriasis, revealing the close connection between the skin and the central nervous system. Reports have even shown that psoriasis symptoms can improve after peripheral nervous system injury.
Some studies have demonstrated that neurotransmitters are involved in the pathogenesis of numerous skin conditions, including psoriasis, addressing the close correlation between the skin and the central nervous system. There are reports showing psoriasis improvement after peripheral nervous system injury.
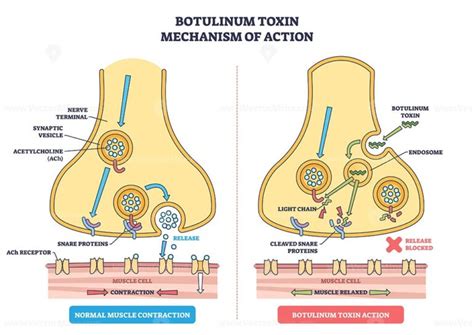
Injection of BoNTs into the skin inhibits the release of SP and CGRP, thereby attenuating dendritic cell activation and interrupting the downstream inflammatory cascade, ultimately leading to the reduction of keratinocyte hyperproliferation and clinical improvement of psoriatic lesions.
Proof-of-Concept Study: Botulinum Toxin for Plaque Psoriasis
A team of researchers conducted a proof-of-concept study of botulinum toxin in 8 patients with stable plaque psoriasis and some lesions that were not responsive to therapy. In the case of each patient, the investigators selected up to 2 plaques with a maximum diameter of 5cm². Participants received a single injection of botulinum neurotoxin A (BoNT-A) at a dilution of 5 units per cm² with a maximum of 50 units.
This is a proof-of-concept study of botulinum toxin and psoriasis, involving eight patients with stable and recalcitrant plaques of psoriasis vulgaris. The lesions were 5 cm² at the maximum. Botulinum toxin Dysport (Ipsen Biopharm, Wrexham, UK), 5 units per cm², was administered in one subcutaneous application. Patients were then evaluated at 2 and 4 weeks after treatment.
The off-label use of abobotulinumtoxinA to treat the patient did not require IRB approval, as it was not initiated as a research study. No cutaneous or muscular adverse events were noted at the time of injection or during the follow-up period. Within three weeks of injection, the patient reported an improvement in plaque severity and complete remission of the treated lesional plaque was noted and sustained until 7 months post-injection. At 8 months post-injection, the lesion recurred in the same location. Concurrent with this, the patient experienced an unrelated outbreak of cutaneous HSV on her right buttock at a previously established site.
Study Findings and Clinical Improvement
At 4 weeks after treatment, researchers reported that the total clinical score was 4.92, a difference of over 3 points revealing significant clinical improvement. All of the parameters evaluated, including desquamation, erythema, and infiltration, for the TCS score were improved. Especially important was the improvement in erythema and infiltration of the evaluated lesions, according to the study’s authors.
“Our results indicated a substantial improvement in all patients, 4 weeks after treatment, with no significant side effects,” stated the researchers. Furthermore, no adverse events were reported, and no adverse events were related to botulinum toxin injection. Nonetheless, the latest findings indicate great promise for botulinum toxin as a psoriasis treatment.
“Our study showed a significant improvement of 38.5% of mean difference (P = .001) of the TCS score following a single dose of BoNT, documented by photographic evaluation,” the study’s authors explained. These results are concordant with other studies that have shown an improvement of psoriasis plaques following BoNT injections.
“Our results indicated a substantial improvement in all patients, 4 weeks after treatment, with no significant side effects. Our study showed a significant improvement of 38.5% of mean difference (P = .001) of the TCS score following a single dose of BoNT, documented by photographic evaluation,” the study’s authors explained. These results are concordant with other studies that have shown an improvement of psoriasis plaques following BoNT injections.
Use of botulinum neurotoxin A (BoNTA) for treating inflammatory skin disease is an underexplored area in medical dermatology. Preclinical mouse studies have demonstrated efficacy of abobotulinumtoxinA in improving psoriasiform skin inflammation. We describe sustained local clearance of a psoriasis plaque in a patient following a single off-label injection of intradermal abobotulinumtoxinA.
A 75-year-old Hispanic woman presented to a private Dermatology clinic with chronic mild-to-moderate plaque psoriasis (PASI 6.1) that had been treated in the past with 0.05% fluocinonide solution to the scalp, and 0.05% clobetasol propionate cream to the active lesions on the body. Multiple well-circumscribed ~1-6 cm white scaly plaques were concentrated on her elbows, forearms, scalp, upper back and gluteal region. The patient had been using topical steroid therapy intermittently on difficult to reach symptomatic plaques but complained about trouble seeing and reaching the plaque on her back/buttocks to apply topical steroids.
Here, we report local plaque remission with a single intradermal treatment of abobotulinumtoxinA (Dysport®) totaling 30 units, the equivalent of ~10-15 units of onabotulinumintoxinA (BOTOX®). To our knowledge, this the first report of efficacy in psoriasis patients of abobotulinumtoxinA-induced skin improvement. This is similar to our prior observations of local skin improvement following intradermal injection in the KC-Tie2 mouse, wherein a single injection lead to disease improvement within 2 weeks, concurrent with decreases in CD4+ and CD11c+ skin-infiltrating immune cells.
The observed timeframe for psoriasis improvement and recurrence are similar to what is known regarding cosmetic use of BoNTA, specifically with respect to glabellar line improvement following intramuscular injection at similar doses (20U).
Review of Existing Literature and Animal Studies
A literature search on the subject of botulinum toxin treatment in psoriasis found 15 relevant articles, 11 on human subjects and 4 on animal studies. Of the human data, eight were clinical trials and three were single case reports. Seven out of eight clinical trials, all open-label, reported improvement in psoriasis following intradermal or subcutaneous botulinum toxin injections. One double-blind, placebo-controlled study, which used a smaller dose than the open-label studies, did not note a healing effect.
Animal studies have shown that injection of botulinum toxins in the skin heals psoriatic skin lesions and can reduce the level of interleukins (ILs) and cytokines as well as inflammatory cells in psoriatic plaques.
Dysregulation of the immune response in psoriasis. From Sieminska et al.-Clin Rev Allergy Immunol 2024 [8].
These results are concordant with other studies that have shown an improvement of psoriasis plaques following BoNT injections.
Potential Mechanisms of Action
The skin affected by psoriasis has more nerve fibers and an elevated level of calcitonin gene-related peptide (CGRP), which plays a role in inflammation. Research suggests that Botox inhibits the release of CGRP, which may be useful as a supplemental therapy for people with psoriasis.
There have been numerous reports of psoriasis remission following nerve injury, nerve blockade, or loss of innervation, suggesting a contributory role for cutaneous nerves in sustaining psoriasis pathogenesis. Recently, we identified the importance of cutaneous sensory nerves, specifically nerve-derived CGRP and SP in sustaining psoriasiform skin inflammation in the KC-Tie2 mouse model, by surgically eliminating the nerves or pharmacologically inhibiting these peptides. Botulinum neurotoxin type A (BoNTA) is best known for its inhibition of cholinergic neurotransmission at the neuromuscular junction, however it is equally efficacious at inhibiting nerve-derived release of SP and CGRP.
We recently validated the ability of a single intradermal injection of BoNTA to exert similar levels of phenotype improvement. Two prior reports have suggested that onabotulinumtoxinA (BOTOX®) can improve inverse psoriasis of the axilla and inframammary regions at doses between 50-100 total units/site.
Safety and Side Effects
“Our results indicated a substantial improvement in all patients, 4 weeks after treatment, with no significant side effects,” stated the researchers. Furthermore, no adverse events were reported, and no adverse events were related to botulinum toxin injection.
In most cases, individuals choose to get Botox injections as a way to reverse the physical effects of aging. If you're interested in discussing this or other anti-aging solutions, contact Dr. People living with psoriasis may choose to undergo cosmetic procedures such as Botox, permanent makeup, and tattoos. These procedures carry risks and may cause flare-ups.
Botox injections, microblading, and lip blushing are not necessarily discouraged for people with psoriasis, but these procedures do carry risks. If you have psoriasis and plan to have cosmetic procedures, it’s helpful to learn about their potential risks, any special considerations, and how to speak with your provider about psoriasis.
In the prescribing information for Botox cosmetic injections, psoriasis is not listed as a condition that should prevent their use. However, the prescribing information states that Botox injections should not be given in areas with pre-existing conditions. Botox injections should also not be given in any areas of existing inflammation.
On the other hand, it has been reported that psoriasis has formed at the site of Botox injections. The prescribing information for Botox cosmetic injections notes that an eruption of psoriasis is a possible adverse reaction.
None of the medications that are known to interact with Botox cosmetic injections are specific to psoriasis. Aminoglycosides, a broad-spectrum antibiotic, anticholinergic drugs, and muscle relaxants are potential interactants. All medications, including over-the-counter products, have the potential for side effects and interactions. It’s a good idea to speak with a healthcare professional before trying a new treatment.
Considerations for Cosmetic Procedures and Psoriasis
People living with psoriasis may choose to undergo a variety of cosmetic procedures. Botox injections, microblading, and lip blushing are not necessarily discouraged for people with psoriasis, but these procedures do carry risks.
If you have psoriasis and plan to have cosmetic procedures, it’s helpful to learn about their potential risks, any special considerations, and how to speak with your provider about psoriasis.
Half of the people living with psoriasis experience psoriasis on the face. Most commonly, this can occur on the skin in the area between the nose and the top lip, the eyebrows, the upper part of the forehead, and the hairline. Facial treatments can sometimes be difficult for people living with psoriasis, as some products can irritate the skin.
People with psoriasis should avoid or limit the use of creams and lotions that contain dyes, fragrances, harmful chemicals, and some essential oils. Even products that are marketed for sensitive skin may still be irritating for people with psoriasis. Any irritation to the skin can cause psoriasis to flare. When psoriasis develops at the sites of irritation, it’s known as the Koebner phenomenon. It’s a good idea to work with a dermatologist to discuss skin care products appropriate for your skin situation.
During a facial treatment, the aesthetician should approach the area with psoriasis very gently, as the skin in this area is very sensitive.
Both microblading and lip blushing are forms of permanent makeup. This is a form of tattoo in which a needle is used to insert colored ink into the skin to give the appearance of permanent eyebrows (for microblading) or lip color (for lip blushing). Although tattooing is not strictly banned for those living with psoriasis, it comes with risks. Consider refraining from getting a tattoo when you’re receiving immunosuppressive treatments or when you’re in an active stage of psoriasis.
Risks of tattoo procedures include infections, serious illness like HIV or hepatitis, allergic reactions, scarring, redness, bumps, and an increased risk of sunburns, swelling or burning at the site of the tattoo during MRI scans, and masking signs of skin cancers. Another known risk from tattooing procedures is the Koebner phenomenon. This occurs when new psoriasis plaques appear on skin that was previously unaffected. This affects roughly 25% of people with psoriasis who experience trauma to the skin. Tattooing is considered trauma to the skin. The National Psoriasis Foundation notes that if you get a tattoo, there’s a significant risk that psoriasis may flare in the tattooed area. In addition, new psoriasis spots may appear at the site of a new tattoo.
Permanent makeup is a type of tattoo procedure that involves injecting ink into the skin to give the appearance of makeup, such as eyeliner, lipliner, filled-in eyebrows, and other forms of makeup. Those with psoriasis should be aware that any permanent makeup procedure is a form of tattoo, and these procedures come with risks. Permanent makeup uses colored ink injected into the skin to give the appearance of makeup. But no ink has been approved by the Food and Drug Administration (FDA) for injection into the skin. Injecting ink into the skin can cause skin injury. This can then cause a flare. It’s also possible for psoriasis to develop in areas where the skin has been injected.
The American Academy of Dermatology recommends that any cosmetic procedure should be done by a physician like a board-certified dermatologist. Before undergoing any kind of cosmetic procedure, it’s important to ask questions. These may include: What qualifications does this professional have? How many of these procedures have they completed previously? Is it possible to see before-and-after photos of previous patients? What results should you expect? What are the risks of the procedure?
If you choose to see a cosmetologist for a facial or other treatment, it’s a good idea to let them know about psoriasis and any active flares that may be present. Explaining that the skin can be very sensitive due to psoriasis may be helpful. It may also be a good idea to ask what kind of products will be used, remembering that some ingredients may be irritating for the skin and could trigger a flare.
Future Directions for Botulinum Toxin Therapy
Further investigation of this therapeutic method is necessary, especially trials including a larger and more diverse patient cohort.
What role can genetics play in future psoriasis treatment? - Professor Jonathan Barker
Michalek I., Loring B., John S. A systematic review of worldwide epidemiology of psoriasis. J. Eur. Acad. Dermatol. Venereol. 2016;31:205-212.
Paller A.S., Singh R., Cloutier M., Gauthier-Loiselle M., Emond B., Guerin A., Ganguli A. Prevalence of Psoriasis in Children and Adolescents in the United States: A Claims-Based Analysis. J. Drugs Dermatol. JDD.
Armstrong A.W., Read C. Pathophysiology, Clinical Presentation, and Treatment of Psoriasis: A Review. JAMA. 2020;323:1945-1960.
Guo J., Zhang H., Lin W., Lu L., Su J., Chen X. Signaling pathways and targeted therapies for psoriasis. Signal Transduct. Target. Ther.
Lee H.-J., Kim M. Challenges and Future Trends in the Treatment of Psoriasis. Int. J. Mol. Sci. 2023;24:13313.
Joseph T, Kurian J, Warwick DJ, Friedmann PS. Unilateral remission of psoriasis following traumatic nerve palsy. Br J Dermatol.
Saraceno R, Kleyn CE, Terenghi G, Griffiths CE. The role of neuropeptides in psoriasis. Br J Dermatol.
Peng Chen Z, Morris JG Jr, Rodriguez RL, Shukla A, Tapia-Núñez J, Okun M. Emerging opportunities for serotypes of botulinum neurotoxins. Toxins (Basel).
Wollina U. Botulinum toxin: non-cosmetic indications and possible mechanisms of action. J Cutan Aesthet Surg.
Messikh R, Atallah L, Aubin F, Humbert P. Botulinum toxin in disabling dermatological diseases. Ann Dermatol Venereol.
tags: #botox #for #scalp #psoriassis