Spitzoid melanoma is a distinct subtype of melanoma characterized by histological and cytological features that resemble those of a Spitz nevus. While often challenging to differentiate from its benign counterpart, Spitzoid melanoma represents a malignant neoplasm with the potential for aggressive behavior and metastasis.
Understanding Spitzoid Melanoma
Spitzoid melanoma is a type of skin cancer that arises from melanocytes, the cells responsible for producing pigment. It is distinguished by its histological appearance, which shares similarities with Spitz nevi, a type of mole typically seen in children. However, unlike benign Spitz nevi, Spitzoid melanoma is a malignant condition that requires prompt diagnosis and treatment.
The term "Spitzoid" refers to the characteristic morphology of the melanocytes, which can be epithelioid (resembling epithelial cells) or spindle-shaped. These cells can grow in nests or fascicles within the skin. The resemblance to Spitz nevi, first described by Sophie Spitz in 1948, initially led to confusion, as she termed them "juvenile melanoma." However, it became evident that while many of these lesions in children behaved benignly, some did not, and true melanomas with Spitzoid features could occur, particularly in adults.
Clinical Presentation
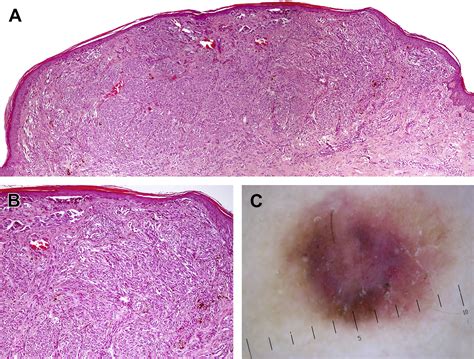
The clinical presentation of Spitzoid melanoma can be varied and often mimics that of a benign Spitz nevus, making visual diagnosis difficult. It typically appears as a solitary growth, often on the extremities (arms and legs) or face, though it can occur elsewhere. Unlike conventional melanomas, Spitzoid melanomas are frequently amelanotic, meaning they lack significant pigmentation, appearing pink, reddish, or skin-colored. However, they can also be pigmented, ranging from brown to black or even blue.
Key clinical features that may raise suspicion for Spitzoid melanoma include:
- Rapid growth over a period of months.
- A lesion that is changing in size, shape, or color.
- A nodule or papule that is slightly pedunculated.
- Lack of typical melanoma features like asymmetry, irregular borders, and multiple colors (though these can sometimes be present).
Dermoscopy, a non-invasive imaging technique, can aid in diagnosis by revealing specific patterns. For amelanotic melanomas, dermoscopic features such as structureless zones with blue, gray, or white colors can be indicative of malignancy. However, dermoscopic findings can overlap with those of benign Spitz nevi, necessitating further investigation.
Histopathological Features and Diagnostic Challenges
The histopathological diagnosis of Spitzoid melanoma hinges on identifying malignant features within a lesion that otherwise resembles a Spitz nevus. This distinction is often challenging due to overlapping criteria.
Key Histopathological Distinctions:
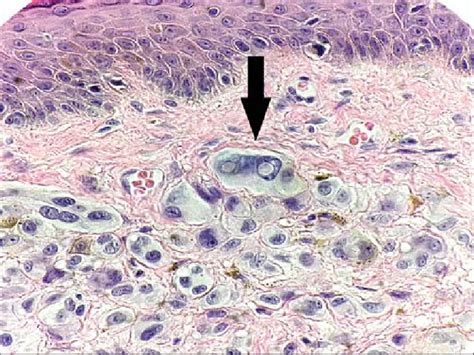
- Cellular Morphology: Both Spitz nevi and Spitzoid melanomas are characterized by large epithelioid and/or spindle-shaped melanocytes.
- Architecture: Spitzoid melanomas often exhibit architectural asymmetry, lack of circumscription, and a dense proliferation of melanocytic nests or sheets with a nodular, expansile appearance.
- Maturation: A lack of maturation of melanocytes with descent into the dermis is a significant indicator of malignancy in Spitzoid melanoma, whereas benign Spitz nevi typically show maturation.
- Mitotic Activity: The presence of numerous mitotic figures, particularly atypical mitoses or mitoses found deep within the dermis, strongly suggests Spitzoid melanoma. Benign Spitz nevi have fewer, non-atypical mitoses, often located in the upper portion of the lesion.
- Depth of Invasion: Deeper invasion into the subcutaneous fat is a critical marker of malignancy in Spitzoid melanoma.
- Other Malignant Features: Ulceration of the epidermis, significant nuclear pleomorphism, and increased cellularity can also be present in Spitzoid melanoma.
The classification of "atypical Spitzoid neoplasm" or "atypical Spitz tumor" is used for lesions that possess features intermediate between a typical Spitz nevus and Spitzoid melanoma, making a definitive diagnosis difficult. These lesions represent a diagnostic challenge for dermatopathologists, as they may have variable potential for malignant progression.
Role of Immunohistochemistry and Molecular Testing
Given the diagnostic difficulties, immunohistochemistry (IHC) and molecular testing play a crucial role in differentiating Spitzoid melanoma from benign Spitz nevi and atypical Spitzoid neoplasms.
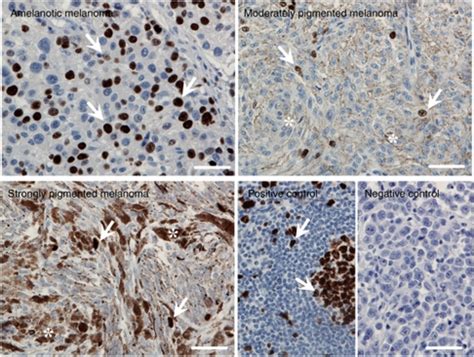
Immunohistochemistry:
- S100: A sensitive marker for melanocytic lesions, but not specific for melanoma.
- HMB-45: Typically shows uniform staining in Spitzoid melanoma, whereas benign Spitz nevi may exhibit a gradient of staining or loss of staining in the deep dermal component.
- Melan-A (MART-1): Another marker for melanocytes that can aid in diagnosis.
- Ki-67: A proliferation marker; higher Ki-67 indices are often seen in Spitzoid melanoma.
- p16: Most benign nevi retain p16 expression, while it may be lost in melanoma.
- S100A6: Often positive in Spitz nevi but can show different patterns in melanoma.
Molecular Testing:
Identifying specific genetic alterations has become increasingly important for accurate diagnosis. Mutations in genes such as BRAF, NRAS, HRAS, and TERT promoter mutations have been studied. Oncogenic fusions involving receptor tyrosine kinases (e.g., ALK, ROS1, NTRK) have also been identified in Spitz tumors. Next-generation sequencing (NGS) and proteomic analyses are powerful tools that can help identify driver genetic alterations, providing greater diagnostic accuracy, especially in challenging cases.
Demographics and Prognosis
While Spitz nevi are most common in children and young adults, Spitzoid melanoma can occur at any age, though it is more frequently diagnosed in adults. Studies suggest that Spitz nevi in individuals in their 20s and 30s may have a higher likelihood of malignancy. The prognosis for Spitzoid melanoma is generally better when detected and treated early, with survival rates strongly correlated with tumor thickness and the extent of spread (metastasis) at the time of diagnosis. Early detection and intervention are crucial for improving outcomes.
Treatment and Management
The treatment of Spitzoid melanoma is primarily surgical excision. The extent of the surgery depends on the tumor's stage, depth, and the presence of metastasis. This typically involves removing the entire lesion with a margin of healthy tissue. For thicker tumors, a sentinel lymph node biopsy may be recommended to assess for spread to nearby lymph nodes. Other treatment modalities, such as radiation therapy, immunotherapy, and chemotherapy, may be considered in advanced cases or for managing metastasis, although their roles are still being defined for this specific subtype of melanoma.