Pityriasis rosea is a common, self-limiting, inflammatory skin condition that typically manifests as a distinctive rash. It is most frequently observed in adolescents and young adults, though individuals of all ages can be affected.
Understanding the Pityriasis Rosea Rash
Herald Patch
The condition often initiates with the appearance of a single, large, oval-shaped, pink or red patch, known as the herald patch. This initial lesion typically presents on the chest, back, or abdomen.
Secondary Rash
Within one to two weeks following the herald patch, a secondary rash emerges, characterized by smaller, more numerous, oval patches. These lesions are often distributed in a pattern that follows the lines of the ribs on the back, creating a visual resemblance to a "Christmas tree" formation.
Characteristics of Skin Lesions
The patches associated with pityriasis rosea are generally flat or slightly raised, featuring a fine, scaly surface. A characteristic feature observed in many cases is a collarette scaling, where the edges of the scale are attached peripherally and lifted near the center of the lesion.
Potential Causes and Etiology
Viral Infection Link
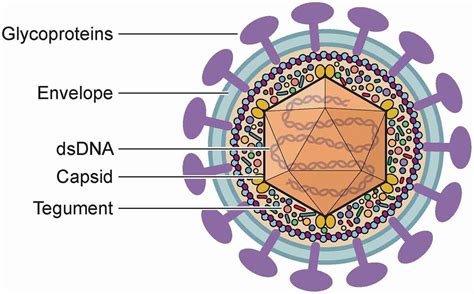
While the precise cause of pityriasis rosea remains unknown, it is widely believed to be associated with viral infections. Specifically, research suggests a potential link to the human herpesvirus 6 (HHV-6) and human herpesvirus 7 (HHV-7). It is important to note that these strains are distinct from the herpes viruses responsible for cold sores or genital herpes.
Other Contributing Factors
Features such as seasonal variation and community clustering suggest an infectious origin for pityriasis rosea. While bacterial agents have not been definitively linked, infections from viruses, bacteria, and spirochetes have been considered. Non-infective causes like atopy and autoimmunity have also been explored. Additionally, pityriasis rosea-like eruptions have been reported following vaccinations and the administration of certain medications, including gold compounds, captopril, barbiturates, and isotretinoin, among others.
Diagnosis and Clinical Presentation
Clinical Examination
The diagnosis of pityriasis rosea is primarily established through a thorough clinical examination, focusing on the characteristic appearance of the rash and the patient's medical history. There are no non-invasive tests that can definitively confirm the condition.
Atypical Presentations
Pityriasis rosea can sometimes present atypically, making diagnosis challenging. This may occur when the typical herald patch is absent, or when there are variations in the morphology, size, or distribution of the lesions. These atypical forms can include generalized papular pityriasis rosea, lichenoid pityriasis rosea, erythema multiforme-like pityriasis rosea, follicular pityriasis rosea, inverse pityriasis rosea, acral pityriasis rosea, unilateral pityriasis rosea, Blaschkoid pityriasis rosea, limb-girdle pityriasis rosea, mucosal involvement, and localized pityriasis rosea.
Differential Diagnosis
It is crucial to differentiate pityriasis rosea from other conditions that may present with similar rashes. These include, but are not limited to, secondary syphilis, dermatophytosis (fungal infections), guttate psoriasis, nummular eczema, pityriasis lichenoides chronica, cutaneous T-cell lymphoma, erythema annulare centrifugum, erythema chronic migrans, erythema multiforme, Kaposi sarcoma, lichen planus, parapsoriasis, and pityriasis alba.
Treatment and Management
Supportive Care
Since pityriasis rosea is a self-limiting condition, it typically resolves on its own without the need for specific medical treatment. The primary goal of management is often to alleviate symptoms, particularly itching.
Symptom Relief
For patients experiencing mild to severe itching, which can occur in up to 25% of cases, various supportive measures can be beneficial. These include the use of emollients, antihistamines, and topical corticosteroids to reduce inflammation and relieve pruritus. In some instances, oral steroids may be considered for severe itching.
Medications and Therapies
While not always necessary, certain treatments may help in faster resolution of lesions and symptom relief. Macrolides and acyclovir have shown potential in this regard. Additionally, narrowband ultraviolet B (UVB) phototherapy is another therapeutic option that has demonstrated favorable results by modulating the immune response in the skin.
Prognosis and Complications
Self-Limiting Course
Pityriasis rosea typically follows a benign and self-limiting clinical course. The rash commonly resolves spontaneously within approximately 6 to 10 weeks, and in most cases, heals without scarring. Recurrence of pityriasis rosea outside the acute phase is rare, estimated at 1-3%.
Potential Complications
Although generally harmless, some complications can arise in rare instances. These may include:
- Superimposed bacterial infection: Scratching the affected skin can lead to secondary bacterial infections, causing pain, redness, and pus.
- Itching, discomfort, and impaired quality of life: Intense pruritus, particularly in the early stages, can disrupt sleep and affect daily life.
- Hyperpigmentation: In some individuals, especially those with darker skin tones, the rash may leave behind patches of discolored skin (lighter or darker), which can take several months to fade.
- Pregnancy-related risks: There are reports suggesting a link between pityriasis rosea during pregnancy, particularly in the first trimester, and an increased risk of spontaneous abortion or premature birth. However, the definitive causal relationship is not fully established.
Deterrence and Patient Education
Patient education is a vital aspect of managing pityriasis rosea. Individuals should be informed about the benign and self-limiting nature of the condition. Advice typically includes avoiding harsh soaps, hot water, and excessive sun exposure, as these can worsen the rash. Wearing loose-fitting clothing and avoiding activities that cause excessive sweating are also recommended. Patients should be encouraged to seek medical attention for severe symptoms, such as intense itching, pain, or fever.
Is Pityriasis Rosea Contagious? Separating Fact from Fiction 🤔
tags: #herpesvirus #7 #pityriasis #rosea