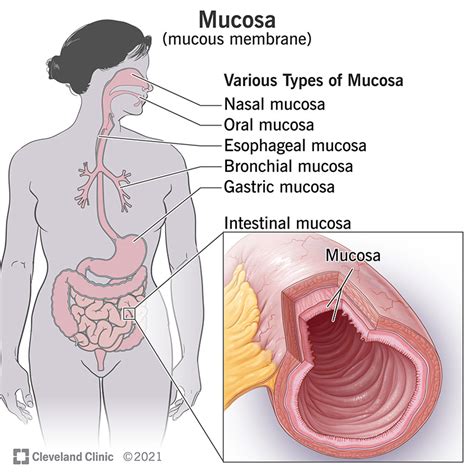
Oral mucosal melanoma is a rare and aggressive form of melanoma, accounting for only about 1% to 3% of all melanoma diagnoses. It originates from melanocytes, the pigment-producing cells, located in the mucous membranes that line various internal body cavities. Unlike cutaneous (skin) melanoma, oral mucosal melanoma is not linked to sun exposure or UV radiation. Its development in less visible areas often leads to delayed diagnosis, making treatment more challenging.
Understanding Mucosal Melanoma
Mucosal melanomas can occur anywhere mucous membranes are present, including the head and neck region (nasal cavity, sinuses, mouth, throat), the anorectal area, the vulva, vagina, cervix, and the urinary tract. The specific symptoms experienced depend on the location of the melanoma.
Types of Head and Neck Mucosal Melanoma
Within the head and neck region, mucosal melanoma can manifest in several ways:
- Oral mucosal melanoma: This type arises in the mouth, including the lips.
- Sinonasal mucosal melanoma: This occurs in the nasal passages or sinuses.
- Pharyngeal/laryngeal mucosal melanoma: This affects the throat and is the least common type within the head and neck.
Causes and Risk Factors
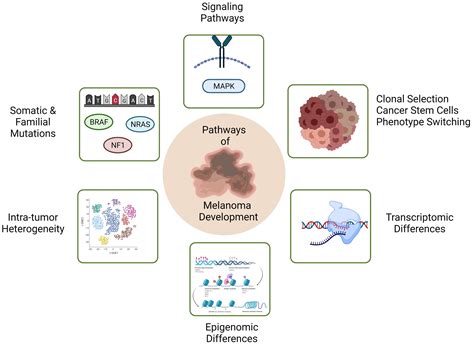
The exact causes of mucosal melanoma remain largely unknown, and unlike skin melanoma, it is not associated with sun exposure. While some studies have suggested potential links to factors like smoking, ill-fitting dentures, or exposure to certain carcinogens (tobacco and formaldehyde) for oral and sinonasal mucosal melanoma, further research is needed to confirm these associations. Genetic mutations, specifically in the KIT and BRAF genes, have been identified in a small percentage of mucosal melanoma cases. KIT gene mutations are found in 7% to 17% of all mucosal melanomas, and even higher in those affecting the vagina and vulva (around 30%). BRAF mutations are less common, occurring in 3% to 15% of mucosal melanomas, compared to up to 80% in cutaneous melanomas.
Symptoms of Oral Mucosal Melanoma
Symptoms of mucosal melanoma can be subtle and easily mistaken for less serious conditions, contributing to delayed diagnosis. It is crucial to consult a healthcare professional for any persistent, unexplained symptoms.
Symptoms by Location:
Head and Neck Region:
- Oral mucosal melanoma:
- A lump on the tongue or in the mouth that grows over at least three weeks, potentially bleeding or being darkly pigmented.
- A mouth ulcer that does not heal within three weeks.
- Mouth pain.
- Bleeding in the mouth.
- Dentures that no longer fit properly.
- Sinonasal mucosal melanoma:
- Repeated nosebleeds from one nostril for at least three weeks.
- A persistent blockage in one nostril for a minimum of three weeks that does not improve with nasal drops.
- Continuous runny nose.
- Facial pain.
- Pharyngeal/laryngeal mucosal melanoma:
- Unexplained hoarseness that persists for over three weeks.
- Swollen glands in the neck that do not improve within three weeks.
- Trouble swallowing (dysphagia).
- A mass or lump on the outside of the neck.
Other Locations:
- Anorectal mucosal melanoma: Pain, a mass or lump, bleeding, constipation, or itchiness in the anus or rectum.
- Vulvovaginal mucosal melanoma: Vaginal bleeding outside of normal patterns, vaginal pain, unusual or bloody vaginal discharge, a lump or growth in the vagina or vulva, or persistent itching.
- Urinary tract mucosal melanoma: Urinary symptoms or blood in the urine.
It is important to note that symptoms like mouth ulcers, nosebleeds, or hoarseness can be indicative of many other less serious conditions. However, if these symptoms persist for more than three weeks or are concerning, seeking medical attention is vital.
Richard Joseph on Mucosal Melanoma
Diagnosis and Staging
Diagnosing mucosal melanoma involves a thorough clinical examination, evaluation of symptoms, and often, imaging scans to determine the extent of the disease. A biopsy is the gold standard for confirming the diagnosis. This procedure involves taking a small tissue sample under local anesthesia, which is then analyzed by a pathologist to identify cancerous cells. The results of a biopsy typically take a few weeks. If the diagnosis is confirmed, further tests are performed to stage the melanoma, which helps guide treatment decisions.
Staging for Head and Neck Mucosal Melanoma
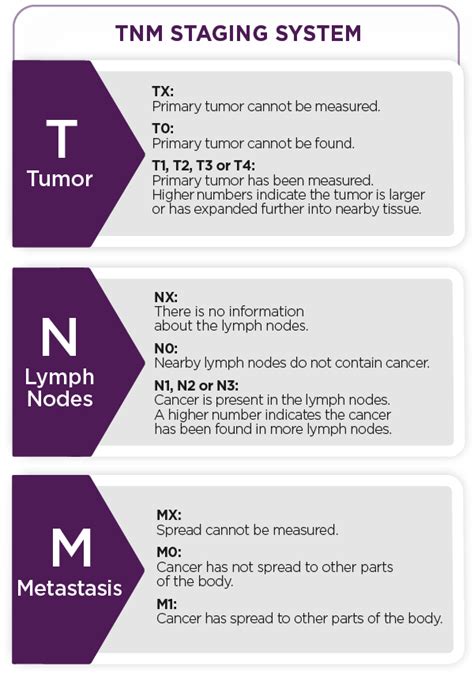
The staging system commonly used for head and neck mucosal melanoma is the American Joint Committee on Cancer (AJCC) Tumour, Node, and Metastasis (TNM) classification:
- T1: Tumors limited to the mucosa, regardless of thickness or greatest dimension.
- T2: Tumors involving the mucosa and submucosa.
- T3: Tumors limited to the mucosa and immediately underlying soft tissue, regardless of thickness or greatest dimension. For example, polypoid nasal disease, pigmented or non-pigmented lesions of the oral cavity, pharynx, or larynx.
- T4: Moderately advanced or very advanced disease.
- T4a: Moderately advanced disease. Tumor involving deep soft tissue, cartilage, bone, or overlying skin.
- T4b: Very advanced disease. Tumor involving, for example, nerves, arteries, the brain, and skull.
- N0: No regional lymph node metastasis.
- N1: Metastasis in regional lymph node(s).
- M0: No distant metastasis.
- M1: Distant metastasis.
Unlike cutaneous melanomas, Clark's levels, which describe the depth of invasion into skin layers, are not applicable to oral mucosal melanomas due to anatomical differences in the oral mucosa. Tumor thickness or volume may serve as a more reliable prognostic indicator.
Treatment Options
The primary treatment for mucosal melanoma is usually surgery, performed by surgeons experienced in complex head and neck procedures, often in specialized centers. If the melanoma has spread to other parts of the body, other treatments may be offered, including immunotherapy or participation in a clinical trial.
Other potential treatments include:
- Radiation therapy: While melanoma is classically not very sensitive to radiation, it can sometimes be used to improve local control and survival, especially in complex areas like the head and neck.
- Chemotherapy: Drugs like dacarbazine and platinum analogs have shown limited response. Targeted therapies, such as dabrafenib and vemurafenib, are used for patients with specific BRAF mutations.
- Immunotherapy: This treatment helps the immune system identify and attack cancer cells.
- Targeted therapy: This approach is effective in cases with specific genetic mutations, such as c-KIT mutations, where drugs like imatinib may be beneficial.
- Clinical trials: These offer access to novel treatments and are particularly valuable for rare cancers like mucosal melanoma.
Prognosis
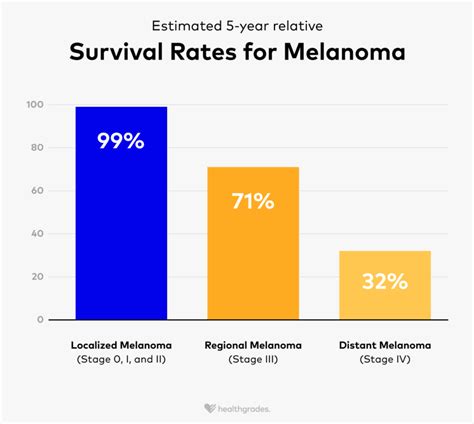
The prognosis for oral mucosal melanoma is generally poorer than for cutaneous melanoma, largely due to delayed diagnosis and its aggressive nature. Around 30% of patients present with lymph node metastasis at diagnosis, which significantly worsens the prognosis. The 5-year survival rate for mucosal melanomas in the head and neck region is approximately 25.5%. Early recognition and treatment are crucial for improving outcomes. Lifelong follow-up is recommended for patients with a history of oral melanoma due to the high risk of recurrence.
Prevention and Patient Education
Preventive strategies for mucosal melanoma are not well-defined due to the unknown causes. However, patient education on regular self-examination of the oral cavity, as well as other mucous membrane areas, is strongly encouraged. Identifying suspicious pigmented or non-pigmented lesions early can significantly improve the chances of successful treatment. Healthcare professionals, including dentists, dermatologists, and general practitioners, play a vital role in educating patients and performing thorough oral examinations during routine appointments.