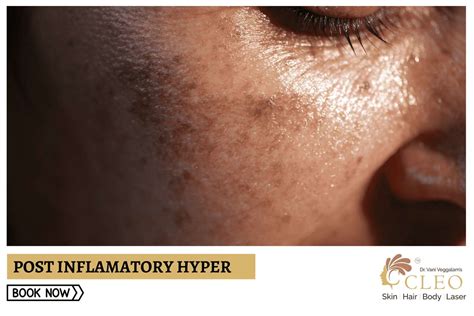
Post-inflammatory hyperpigmentation (PIH) is a temporary pigmentation that follows an injury or inflammatory disorder of the skin. It is characterized by flat, tan, brown, or black spots on the skin. This condition is most commonly observed in darker skin types, where the color tends to be more intense and persist for a longer period than in lighter skin colors. PIH can occur in anyone but is more prevalent in individuals with darker skin.
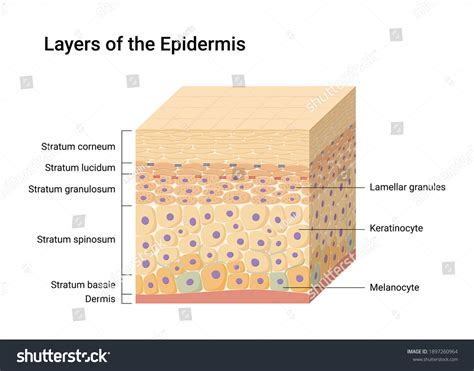
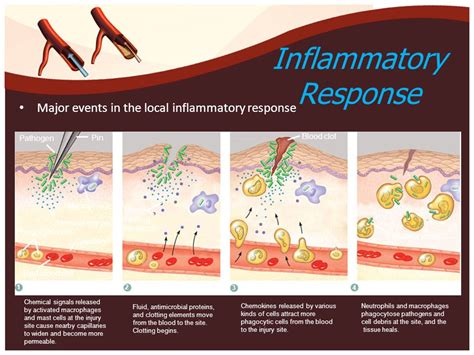
Inflammation, such as that resulting from acne, eczema, lichen planus, or allergic reactions, as well as trauma to the skin from surgery, microdermabrasion, lasers, or chemical peels, triggers the release of inflammatory cells. These cells stimulate melanocytes, the pigment-producing cells in the skin, to produce more pigment. In cases of severe inflammation or trauma, the bottom layer of the epidermis can be disrupted, causing pigment to leak into and become trapped in the dermis. This leads to the characteristic appearance of PIH.
Causes of Post-Inflammatory Hyperpigmentation
The primary cause of PIH is inflammation or injury to the skin. Several factors can contribute to its development:
Inflammatory Conditions:
- Eczema (Atopic Dermatitis): Eczema lesions, which are often itchy and inflamed, can lead to changes in skin pigmentation. Scratching eczema patches can worsen irritation and trigger pigmentary changes. Inflammation during an eczema flare-up causes the body to release cytokines, which in turn stimulate melanocytes to increase melanin production. This increased pigment can be transferred to keratinocytes.
- Acne: Breakouts can cause inflammation that leads to dark spots after the acne lesions heal.
- Lichen Planus: This inflammatory condition can also result in hyperpigmentation.
- Allergic Reactions: Reactions to allergens can cause inflammation and subsequent PIH.
Skin Trauma:
- Surgical Procedures: Incisions and healing from surgery can lead to PIH.
- Cosmetic Procedures: Incorrect use of treatments like microdermabrasion, laser therapy, and chemical peels can cause inflammation and damage, resulting in PIH.
- Burns: Thermal burns can also cause post-inflammatory pigmentation.
It is important to note that in darker skin tones, inflammation is often more difficult to detect as redness is not always apparent. Instead, it may manifest as various stages of hyperpigmentation, making it a more subtle indicator. Another feature of eczema, more commonly found in darker skin, is follicular prominence, where eczema appears as small, itchy bumps or papules, particularly on the trunk and forearms.
Characteristics and Diagnosis of PIH
Post-inflammatory hyperpigmented patches are typically located at the site of the original injury or inflammatory condition after it has healed. The lesions range in color from light brown to black. In some cases, a skin biopsy may be necessary to differentiate PIH from other skin conditions with similar appearances, such as melasma, hyperpigmented pityriasis versicolor, lichen planus (macular variant), amyloidosis (macular variant), and hyperpigmented mycosis fungoides.
Diagnosis is usually made through a careful patient history and physical examination of the skin. Sometimes, the diagnosis is confirmed only after a biopsy.
PIH in Different Skin Types
While PIH can occur in anyone, it is more common and often more pronounced in individuals with darker skin. This is because darker skin types have more active melanocytes and produce more melanin. Consequently, the hyperpigmentation in these individuals tends to be more intense and may persist longer. A UK longitudinal study on ethnic variations in atopic eczema reported that children with darker skin, particularly of African-Caribbean ethnicity, were more likely to develop atopic eczema and were six times more likely to develop severe eczema compared to their white counterparts.
On lighter skin, eczema typically presents as inflamed pink or red patches that are dry and itchy. In contrast, on darker skin tones, these lesions may appear purple, gray, or a darker brown than the surrounding skin. When people with light skin scratch eczema lesions, both hyper- and hypopigmentation can occur, and the subtle changes can make detection difficult.

Specific Considerations with Eczema
When eczema flares up, the body releases cytokines, which cause inflammation. This inflammation triggers the melanocytes to produce more melanin. If the skin is injured by scratching or rubbing, melanin is released, contributing to hyperpigmentation. Post-inflammatory pigmentation can occur even after the eczema flare has subsided, appearing as a darker patch where eczema lesions have healed. This can be frustrating as the darkened patch may linger for months, even if the eczema does not recur in that area.
Lichenification is another consequence of chronic scratching and rubbing associated with eczema. This results in thickened areas of skin with visible scratch marks and increased skin markings. These areas of hyperpigmentation may appear gray on dark skin and dark pink on light skin. Lichenification occurs in all skin types and can become a habit, even when eczema is not actively flaring.
Some individuals with eczema worry that hypopigmentation (lighter patches) might be a side effect of topical treatments, particularly topical steroids. While topical steroids can cause temporary dilation of small blood vessels, this is not permanent skin damage. Another cause of paler patches is pityriasis alba, a mild form of eczema common in children and teenagers. Pityriasis alba is more prevalent in darker skin and often appears after sun exposure, as the hypopigmented areas do not tan, making them more prominent. Pityriasis alba typically presents as one to 20 round or oval patches, mainly on the face, but also on the neck, shoulders, and upper arms. A key difference from eczema is that pityriasis alba is accompanied by little or no itching, although it can coexist with itchy eczema patches.
DERMATOLOGIST ANSWERS YOUR ECZEMA QUESTIONS 🤔@DrDrayzday
Treatments and Management
The main strategy for improving skin pigmentation changes associated with eczema is to treat the underlying eczema and inflammation. While there is currently no specific treatment directly for the pigmentary skin changes themselves, they typically resolve over time.
Sun Protection:
If pigmentation affects an exposed area, daily application of SPF 50+ broad-spectrum sunscreen is crucial. Sun protection is important for people of all skin types as it can prevent PIH from worsening and help it recover. Sunlight stimulates post-inflammatory pigmentation, so covering affected areas and using sun protection is advisable.
Topical Treatments:
A variety of topical treatments are available to lighten hyperpigmented lesions in epidermal hypermelanosis. These may include agents that inhibit melanin production or promote skin exfoliation.
Managing Eczema:
For people with eczema, treating the condition effectively is paramount. This can involve prescription topical steroids, non-steroid creams, and other treatments as determined by a doctor or dermatologist. Using a moisturizing cream or ointment can help address dryness associated with eczema.
Resolution of Pigmentation Changes:
Over time, both hyper- and hypopigmentation associated with eczema will eventually resolve. However, it is important to remember that these pigmentary changes can persist even after the eczema has been successfully treated. Hypopigmentation from eczema typically resolves within 1 year but may take 2â3 years to disappear completely. Hyperpigmentation, while temporary, can persist for months and tends to last longer on dark skin tones.
If a person's eczema or pigmentation changes do not resolve on their own, consulting a doctor or dermatologist is recommended to establish a treatment plan. People concerned about patches of hyper- or hypopigmentation should also speak with a healthcare professional.
tags: #post #inflammatory #hyperpigmentation #eczema