Research breakthroughs are offering patients with atopic dermatitis, commonly known as eczema, an increasing number of treatment options. Atopic dermatitis is a condition that makes the skin itchy and inflamed, and can cause red or darker colored patches during a flare-up. Symptoms can range from mild to severe and may appear and disappear over time.
If you are pregnant and experiencing this itchy, inflamed skin condition, you are not alone, as atopic dermatitis is common during pregnancy. In fact, over half of individuals with eczema develop symptoms for the first time while pregnant. Pregnancy can be a challenging time, marked by swelling, nausea, and extreme fatigue, and skin conditions like eczema can further complicate the experience. It is understandable to be concerned about the safety of treatments for both yourself and your developing baby.
Understanding Eczema During Pregnancy
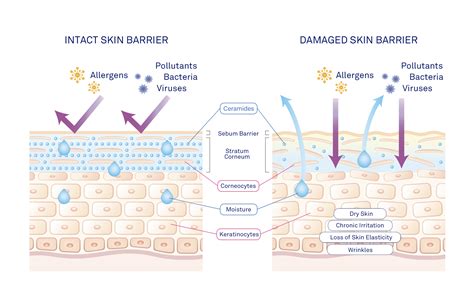
During pregnancy, skin naturally becomes physiologically drier for all women, regardless of their history of atopic conditions. Eczema is characterized by damage to the skin's barrier, leading to moisture loss, dryness, scaling, and increased sensitivity to irritants. This results in dry, scaly, itchy, and red skin. Atopy refers to an immune system issue that predisposes individuals to allergic conditions such as eczema, asthma, and hay fever. You may be able to identify and avoid other triggers that affect you.
Eczema is the most common skin condition that can develop during pregnancy. Some individuals experience eczema symptoms for the first time during pregnancy, while others may have a flare-up of a pre-existing condition. Symptoms are more likely to appear in the first two trimesters. While eczema can be uncomfortable, there is no research indicating that it affects fertility, increases the risk of miscarriage, premature birth, or causes birth differences.
A dermatologist is a medical doctor who specializes in treating the skin, hair, and nails. Your doctor will diagnose eczema by examining your skin. In some cases, a small skin sample, known as a biopsy, may be taken for microscopic examination. If you are taking other medications to treat your eczema, it is crucial to consult your doctor to confirm their safety during pregnancy. This consultation should occur as soon as you begin planning a pregnancy or when you discover you are pregnant. If your eczema began during pregnancy, it typically improves after childbirth.
Treatment Approaches During Pregnancy
There are several ways your healthcare providers may manage your atopic dermatitis during pregnancy. Treatments can be topical, applied directly to the skin, such as moisturizers and creams, or systemic, taken orally or via injection. Generally, topical treatments are considered the first line of defense during pregnancy due to the route of exposure. The developing baby is exposed to substances present in the pregnant woman's bloodstream. Medications taken by mouth are very likely to enter the bloodstream and can potentially cross the placenta to reach the baby. Most topical products are designed so that the skin acts as a barrier, minimizing the amount of product absorbed into the bloodstream and subsequently reaching the baby.
Topical Treatments
Mild, moderate, and potent topical steroids are considered safe for short treatment periods of up to two weeks during pregnancy. It is important to remind patients to use topical corticosteroids as soon as their skin feels itchy or becomes red or rough. Delaying treatment can prolong the time it takes to control eczema. The application amount can remain the same as before pregnancy: one fingertip unit for two palms of the hand, applied once daily, until redness, itching, and roughness subside. Emollients should continue to be used even when the skin appears healthy.
Conversely, it is currently recommended to discontinue the use of tacrolimus during pregnancy. If you have nipple eczema that requires additional treatment to reduce inflammation, usually with topical steroids, follow your healthcare professional's advice. After applying topical steroids, it takes approximately one hour for the skin to absorb them. Therefore, a one-hour gap should be maintained after applying them to the nipple, followed by washing the nipple with emollient before feeding. Some breastfeeding mothers wonder if their diet affects their baby's eczema. Research does not definitively state whether dietary changes in the mother reduce eczema severity in a breastfed child. If you suspect a food allergy, for instance, if your baby reacts after breastfeeding, it could be a response to something you have consumed.
If you had a caesarean section, extra care is needed for your wound. To reduce itching and scarring as it heals, gently apply emollient to the area. Consult your midwife regarding when you can begin this, as it depends on your individual circumstances. It is safe to use emollients while breastfeeding, which can help prevent nipple eczema.
Light Therapy (Phototherapy)
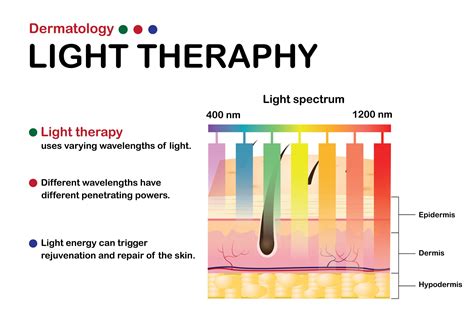
Light therapy, also known as phototherapy, is a treatment option for atopic dermatitis that involves controlled exposure of the skin to ultraviolet (UV) light. Various types of light therapy exist, including narrowband (NBUVB), broadband (BBUVB), UVA, UVA1, full-spectrum light, saltwater bath plus UVB (balneophototherapy), and psoralen plus UVA (PUVA). UV light is the same light emitted by the sun and is not considered radiation.
While research on light therapy during pregnancy is limited, it is not expected to increase the risk of pregnancy complications. Most types of light are not anticipated to be absorbed through the skin and reach the developing baby. However, although NBUVB and BBUVB phototherapy can be used during pregnancy, they may reduce folic acid levels. Folic acid is vital for the baby's development, particularly in the first trimester. It is essential to discuss folic acid supplementation and monitoring with your healthcare provider if you require phototherapy during the first trimester.
To further understand how atopic dermatitis and light therapy might affect pregnancy, MotherToBaby is conducting the Eczema & Pregnancy Study, enrolling pregnant individuals. Participation can contribute to the health of future families.
Sunscreen Use
Your healthcare provider may suggest using sunscreen for additional skin protection after light therapy. Sunscreen ingredients such as avobenzone, homosalate, octisalate, and octocrylene can be absorbed through the skin in small amounts with regular use, especially when applied over large body areas. However, there is no proven increased risk to a pregnancy from using these ingredients. Mineral sunscreens contain zinc or titanium, which are physical blocking agents and remain on the skin's surface. This means they are not absorbed and are not expected to reach the developing baby.
Important Considerations and Recommendations
Consult Your Healthcare Provider: Always discuss any new treatment with your healthcare provider before starting, especially during pregnancy. They can help determine the safest and most effective options for your specific situation.
Alternative Treatments: If light therapy is not suitable for you during pregnancy, there may be other treatment options available to help manage your symptoms. Do not hesitate to explore these with your doctor.
Managing Stress: Stress is a known trigger for eczema in many individuals, and pregnancy can be a source of significant stress. Practicing relaxation techniques such as deep breathing, resting, listening to calming music, and positive self-talk can be beneficial.
Diet and Supplements: A recent Cochrane review found insufficient evidence to recommend specific maternal diets or supplements to prevent atopic eczema in infants. Some studies suggest probiotics may play a role in reducing risk, but the evidence is currently weak, and the most effective strains are unclear. European studies have validated the safety of probiotic and prebiotic intake during pregnancy, which can be used in addition to standard care. Probiotics are beneficial bacteria, with Lactobacillus rhamnosus GG being a relevant strain for eczema. Prebiotics are plant fibers that support probiotic survival.
Breastfeeding and Eczema: Eczema can persist or develop after childbirth. The extra washing and cleaning involved in caring for a newborn can aggravate or cause hand eczema. If you have eczema, it is important to schedule time to manage your treatment regimen alongside caring for your new baby. It is safe to use emollients while breastfeeding, and they can help prevent nipple eczema. If nipple eczema requires treatment with topical steroids, follow your healthcare professional's guidance. After applying topical steroids, wait an hour before breastfeeding. Some breastfeeding mothers wonder if their diet could affect their babyâs eczema. Research does not conclusively show whether changing a motherâs diet reduces the severity of eczema in a breastfed child. If you suspect a food allergy, such as a reaction after breastfeeding, it may be related to something you have eaten.
Genetics and Prevention: If you or your partner have a history of eczema, asthma, or hay fever, it is natural to be concerned about your baby developing these conditions. While atopic eczema has a genetic component, there is no definitive evidence that specific pre-conception or pregnancy-related lifestyle changes can prevent it. While some women experience improvement in their eczema during pregnancy, others find their condition worsens.
Postpartum Care: Eczema can flare up after childbirth. It is crucial to plan for managing your treatment regime alongside the needs of your newborn. For caesarean section wounds, gentle emollient application can help reduce itch and scarring.
Atopic dermatitis can be challenging to manage, particularly during pregnancy. However, options like light therapy offer a potential avenue for relief for many pregnant individuals struggling with this skin condition. Always consult with your healthcare provider to determine the best course of action for you and your baby.