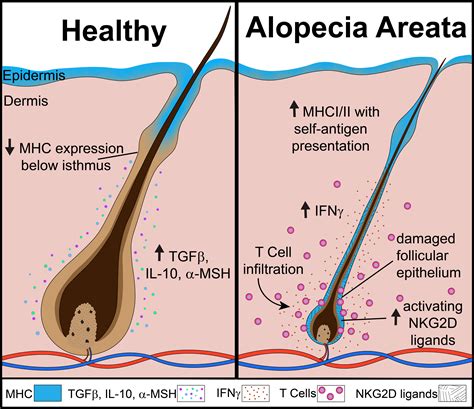
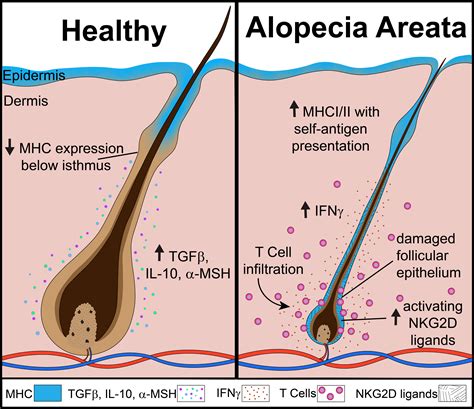
Alopecia areata (AA) is an autoimmune disease that affects approximately 2% of the population, characterized by the immune system attacking the hair follicles, resulting in hair loss. While this hair loss may be undetectable at first, it can become more noticeable as affected regions merge. The condition can be distressing, but various treatments are available to help manage hair loss symptoms.
Effective Treatments for Alopecia Areata
Effective treatments for alopecia areata aim to block the immune system's attack on hair follicles, allowing hair to regrow. It's important to note that not all treatments work for everyone, and finding the right one may require time and patience. Some individuals with mild alopecia areata may opt for no treatment at all.
Corticosteroids
Corticosteroids, also known as steroids, reduce inflammation around hair follicles, which helps hair to grow. They are often used in combination with other alopecia areata treatments.
Intralesional Corticosteroid Injections
The most common treatment for adults with patchy alopecia areata is the intralesional injection of corticosteroids. This involves a very fine needle injecting medication directly into the bald patches on the scalp or face. While some patients find the injections painful, others experience only slight discomfort. New hair growth may be observed within six to eight weeks if the injections are successful. These injections can be repeated every four to six weeks and stopped once hair regrows. However, corticosteroid injections do not prevent further hair loss.
Pulse Corticosteroids
Pulse corticosteroids involve administering a high dose of corticosteroids at regular intervals over a short period. While effective for moderate to severe hair loss, oral steroids can cause side effects such as weight gain, thinning bones (osteoporosis), elevated blood sugar levels, and high blood pressure. Due to these potential side effects, they are not suitable for long-term treatment.
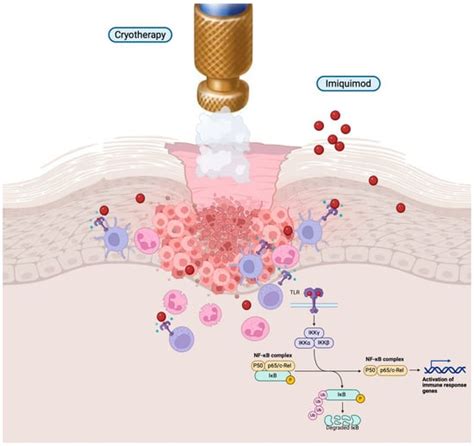
Immunotherapy
Topical Immunotherapy
Topical immunotherapy is considered the most effective treatment for extensive alopecia areata, including alopecia totalis and alopecia universalis. It involves applying chemicals directly to the scalp to elicit an allergic response, stimulating the immune system and boosting hair growth. Chemicals like dinitrochlorobenzene, diphencyprone, and squaric acid dibutyl ester may be used. This treatment, typically recommended and directed by a dermatologist, has shown significant success, with approximately 40% of individuals regenerating scalp hair after about six months. Continuous use is usually necessary to maintain regrowth. However, potential adverse effects include a potentially severe rash, redness, and discomfort where the agent is applied, resembling poison oak or ivy. Some reports indicate that 40 to 55% of patients experience significant regrowth. Persistent dermatitis, severe cervical lymphadenopathy, widespread eczema, blistering, contact leukoderma, and urticarial responses are possible, though uncommon, side effects. Topical immunotherapy may not be readily available everywhere and is not effective for everyone.
Immunotherapy Agent
This type of immunotherapy agent induces an allergic rash (allergic contact dermatitis) at the application site. This alters the immune response around the hair follicles, though the exact mechanism for promoting hair regrowth is not fully understood. The rash can resemble poison oak or ivy. If hair regrowth is successful, ongoing treatment is typically required to maintain it. The treatment can be uncomfortable, causing redness and rash.
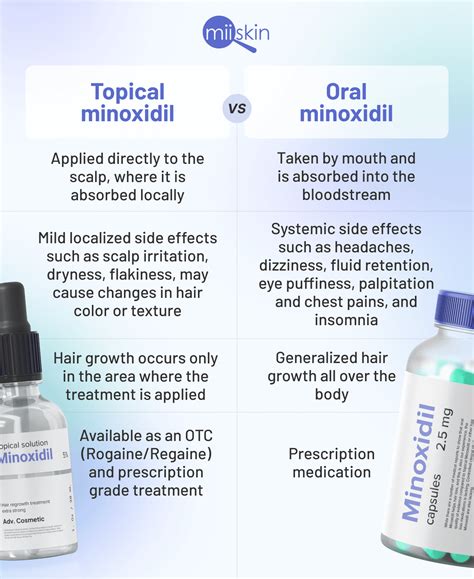
Minoxidil
Minoxidil, commonly known by brand names like Rogaine, is an over-the-counter topical treatment that can help induce hair regrowth in alopecia areata. It is thought to enhance hair growth by stimulating blood flow to hair follicles, awakening dormant follicles, and promoting new hair growth. Minoxidil is available in topical solutions, typically at concentrations of 2% or 5%, and is applied directly to the scalp or other affected areas once or twice daily.
Topical Minoxidil for Alopecia Areata
Topical minoxidil is generally considered best for mild alopecia areata. Studies have demonstrated a dose-response effect; for instance, a study comparing 1% and 5% topical minoxidil showed significantly higher response rates with the 5% formulation in patients with extensive hair loss. The current 2% formulation is most likely to achieve cosmetically acceptable regrowth in those with patchy alopecia areata. Occlusion of the treated area may be necessary to achieve and maintain maximum results. Nonresponders are more likely to have extensive scalp hair loss, but no other clinical features strongly correlate with treatment response. However, increased T cell blastogenesis before treatment might predict response.
Minoxidil and Alopecia Areata: Addressing Myths and Misconceptions
There are several common myths and misconceptions surrounding the use of minoxidil for alopecia areata:
- Myth 1: You need to use it forever. This "rule" primarily applies to androgenetic alopecia (hereditary hair loss). For alopecia areata, it is often possible to stop minoxidil once hair has regrown well, although it may be needed again in the future.
- Myth 2: The bottle says not to use it if I have patches of hair loss. Minoxidil is only FDA-approved for treating genetic hair loss. Its use for alopecia areata is considered "off-label" because it has not undergone the formal FDA approval process for this condition. Companies cannot legally advertise its use for alopecia areata, but physicians can recommend it.
- Myth 3: Minoxidil can cause hair loss. While men and women using minoxidil for androgenetic alopecia may experience initial shedding, this is often a sign that older hairs are being shed to make way for new, stronger ones. In alopecia areata, initial shedding can occur, but it's crucial to distinguish this from a worsening of the disease itself.
- Myth 4: Should I use 2% or 5%? Drops or foam? The choice of minoxidil formulation and strength should be individualized. Consistency in applying the product to the scalp is key. Lower concentrations or different application methods may be recommended for sensitive individuals or those experiencing side effects.
Systemic absorption of topically applied and occluded minoxidil solutions (1% and 5%) has been found to be minimal, with no clinically significant changes in blood pressure, weight, cardiovascular status, or other health markers observed.
Minoxidil as an Adjunct Therapy
While minoxidil may offer only slight benefits when used as monotherapy, it can be a valuable addition to treatment plans involving other agents like topical steroids, steroid injections, anthralin, or diphencyprone. Studies dating back to the 1980s have supported its efficacy in patients with alopecia areata.
What to Expect When Using ROGAINE® Minoxidil Products:
- 1-3 Weeks: Shedding of old, thin hairs to make way for new growth.
- 2-4 Months: Start of hair regrowth, with soft, baby hairs appearing.
- 4-6 Months: Noticeable coverage as hair becomes thicker and fuller.
- 6+ Months: Lasting results with continued twice-daily use to maintain and prevent further loss.
It may take at least 4 months to see results, and individual success can depend on proper application and dosage. A temporary increase in hair shedding during the first few weeks is a good sign, indicating a new growth cycle is beginning. Continued use is necessary to maintain hair regrowth, as stopping treatment will likely lead to the return of normal hair loss patterns within 3 to 4 months.
Hair Loss: Androgenic Alopecia
Other Treatments for Alopecia Areata
JAK Inhibitors
Janus kinase (JAK) inhibitors are immunomodulatory drugs that interfere with signal transmission in the immune system involving Janus kinase proteins. They are considered a first-line treatment for severe forms of alopecia areata, including universalis and totalis. Novel developments in treating alopecia areata are exploring JAK inhibitors, and some may receive FDA approval following clinical trials.
Oral Minoxidil
Oral minoxidil is available in tablet form (2.5 mg, 5 mg, or 10 mg strengths) and may be included in treatment plans for patients with moderate disease, often in conjunction with topical corticosteroids.
Topical Anthralin
Topical anthralin, initially used for psoriasis, has also shown usefulness for mild alopecia areata. It acts as a "scalp sensitizer," causing an irritating reaction that activates the immune system and promotes hair growth. Applied once daily to the scalp and washed off after a specified time, it can lead to rapid hair regrowth within two to three months. However, it can cause irritating dermatitis, and its purple, tar-like consistency may discolor baths and bedsheets. Temporary darkening of lighter skin tones and hair colors may also occur.
Dupilumab (Dupixent)
For individuals with alopecia areata who also have atopic dermatitis or eczema (which affects about one-third of AA patients), dupilumab (Dupixent) is a monoclonal antibody FDA-approved for treating atopic dermatitis in adults and children as young as six months.
Understanding Type 2 Inflammation in Alopecia Areata
Type 2 inflammation plays a significant role in alopecia areata. Immune cells and hair follicles interact through cellular mechanisms that utilize Janus kinase proteins (JAKs) to transmit signals within the immune system. Understanding this interaction is crucial for developing targeted treatments.
Conclusion on Treatment and Future Hope
Alopecia areata can be a challenging condition to manage, but recent scientific advances offer increasing hope for expanded treatment options in the future. While there is currently no single FDA-approved treatment specifically for alopecia areata, novel approaches, such as oral Janus kinase inhibitors, are undergoing clinical trials and may become available.