The calculator below computes the total surface area of a human body, referred to as body surface area (BSA). Direct measurement of BSA is difficult, and as such many formulas have been published that estimate BSA. BSA is often used in clinical purposes over body weight because it is a more accurate indicator of metabolic mass, which represents the body's need for energy. Metabolic mass can be estimated using fat-free mass, where fat-free mass is all of a person's body mass that does not include fat. This includes bones, tendons, inner organs, muscles, blood, nerves, and more.
BSA is also used in various other clinical settings, such as determining cardiac index (to relate a person's heart performance to their body size) or, most commonly, dosages for chemotherapy, a category of cancer treatment. While dosing for chemotherapy is often determined using a patient's BSA, there exist arguments against the use of BSA to determine medication dosages that have a narrow therapeutic index. The therapeutic index is the comparison of the amount of a substance necessary to produce a therapeutic effect to the amount that causes toxicity. If the therapeutic index is too narrow, BSA may not be an accurate enough measure, and there is a risk of causing a toxic rather than therapeutic effect.
There is also evidence that BSA becomes less accurate at the extremes of height and weight, and Body Mass Index (BMI) may be a better estimate in such cases. Below are some of the most popular formulas for estimating BSA, and links to references for each for further detail on their derivations.
Popular BSA Estimation Formulas
Several formulas exist for estimating Body Surface Area (BSA), with varying degrees of accuracy and applicability. Some of the most widely recognized include:
Du Bois Formula
The most widely used of these is the Du Bois formula, which has been shown to be effective for estimating body fat in both obese and non-obese patients, unlike body mass index. This formula was first published by Du Bois D, Du Bois EF in June 1916 in the journal Archives of Internal Medicine.
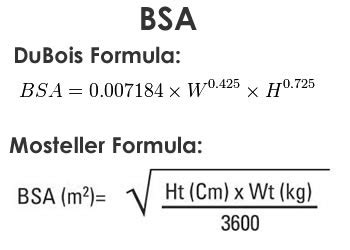
Mosteller Formula
The Mosteller formula, published by Mosteller RD in the New England Journal of Medicine in 1987, is another commonly cited method for estimating BSA.
Boyd Formula
Edith Boyd's work in 1935, published as "The Growth of the Surface Area of the Human Body" as part of the Monograph Series of the Institute of Child Welfare at the University of Minnesota, also provides a method for BSA calculation.
Fujimoto Formula
Studies by Fujimoto S, Watanabe T, Sakamoto A, Yukawa K, and Morimoto K on the physical surface area of Japanese individuals led to the development of calculation formulae in three stages over all ages.
Schlich Formula
Schlich E, Schumm M, and Schlich M proposed a method using 3-D body scans as an anthropometric procedure to determine specific body surface area.
Burn Surface Area Calculation
The total body surface area (TBSA) of a burn is a critical factor in burn assessment, influencing treatment decisions, particularly the volume of fluid resuscitation. Several methods are used to calculate TBSA:
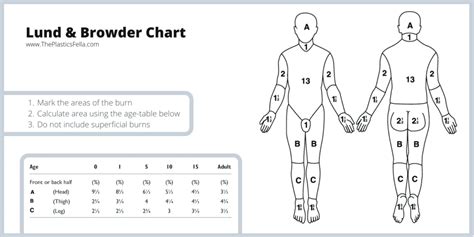
Lund and Browder Chart
The Lund and Browder Chart, first published in 1944, is considered the gold standard for burn surface area calculations due to its established accuracy. Unlike other formulas, it accounts for variations in body shape with age, making it suitable for both adults and children. For example, the area of the head constitutes a larger proportion of total skin area in infants compared to adults, a factor the Lund and Browder chart considers. This method requires knowledge of burn depth and does not include superficial burns in its calculation.
- Positives: High accuracy with less variability compared to other methods like the Rule of Nines.
- Negatives: Difficulties in assessing lateral burns, lack of anatomical landmarks, inability to accurately represent obese individuals, and less efficient than other methods. It also requires knowledge and experience in triaging burn depth.
Wallace Rule-of-Nines
The Wallace Rule of Nines, first described by E.J. Palaski and C.W. Tennison and later published by Wallace in 1951, is a clinically efficient and accurate method for calculating TBSA. It divides the body into percentages of 9%. This method is commonly used in healthcare practice due to its simplicity and proven accuracy for full-thickness and partial thickness burns. It does not include superficial burns in the calculation.
- Positives: Simple to use, easy to remember, and infrequent underestimation of burns.
- Negatives: Can often over-estimate TBSA, potentially leading to over-fluid resuscitation. Accuracy concerns exist for obese and pediatric populations. For infants weighing less than 10 kg, a "Rule of Eights" is a better approximation.
What is Wallace rule of nines?
Palmar Method
The Palmar Method is the simplest technique for estimating a burn's skin percentage. It utilizes the patient's palm, with the palm and digits often considered to represent 1% of the patient's total body surface area, or 0.8% for the palm with digits, and 0.5% for the palm without digits. NICE guidelines recommend using the palm including digits for estimating smaller or scattered burns. However, this method is limited by user and patient variability and has been noted to cause confusion amongst healthcare professionals regarding whether to include digits.
- Positives: Simple and ideal for small and scattered burns.
- Negatives: Limited by user and patient variability, potential for significant estimation errors in larger burns, and confusion regarding the inclusion of digits.
Limitations and Considerations
It is important to note that estimations of burn size can be heavily user-dependent, potentially resulting in over-estimation and significant inter-rater variability, an issue for all traditional burn estimation techniques. Assessment of burn size should not include erythematous (red) areas.
The National Burn Repository indicates that the mean burn size is 13.4% of the total body surface area. For individuals with a narrow therapeutic index, BSA may not be sufficiently accurate for medication dosing, risking toxic effects. Furthermore, at the extremes of height and weight, BSA calculations can become less accurate, with BMI potentially serving as a better estimate.