Untreated tuberculosis (TB) disease poses a greater risk to both the pregnant woman and the fetus than its treatment. If a pregnant woman with TB disease is not treated, the infant may be born with a low birth weight. In rare circumstances, the infant may be born with TB disease. Therefore, health care providers should test pregnant women who are at higher risk of developing TB disease.
Tuberculosis (TB) is caused by a bacterium called Mycobacterium tuberculosis. TB usually affects the lungs but can also affect other parts of the body, such as the brain, kidneys, or spine, and sometimes multiple parts of the body simultaneously. Not everyone infected with TB germs becomes sick; these germs can live in the body without causing illness, which is known as inactive TB. TB germs become active if the immune system cannot stop their growth, leading to active TB disease, where the person feels sick and can spread the germs to others, including their baby, before or after birth.
Symptoms of active TB disease can include feeling weak or sick, weight loss, fever, and night sweats. If TB disease affects the lungs, symptoms may also include coughing, chest pain, and coughing up blood. TB disease can cause death if left untreated.
TB Testing Options During Pregnancy
There are two main types of tests for TB infection: the TB skin test and the TB blood test. Both the TB blood test and the TB skin test are considered safe to use during pregnancy.
The TB Skin Test (Mantoux Test)
The tuberculin skin test (TST), also known as the Mantoux test, is performed to determine if a person has been exposed to tuberculosis (TB). This test involves injecting a small amount of TB protein, called purified protein derivative (PPD), under the top layer of skin on the inner forearm. PPD is derived from tuberculin and is used in standardized testing solutions approved by the FDA.
The injection creates a small bump (wheal) under the skin. A reaction, typically a firm red bump, may indicate infection with TB bacteria. The size of this bump is measured 2 to 3 days after the test to interpret the results. A positive tuberculin skin test signifies the presence of TB germs in the body but does not distinguish between active or inactive TB, nor does it differentiate between a TB infection and a TB vaccination (BCG vaccination).
The TB skin test should be administered and read by a trained health care provider. Training is essential for accurate interpretation. The CDC provides free training materials, including fact sheets, wall charts, and videos, for administering and reading the TB skin test.
Important Considerations for the TB Skin Test During Pregnancy:
- The tuberculin skin test is considered both valid and safe to use throughout pregnancy.
- It helps screen expectant mothers for TB exposure, including latent tuberculosis, which can still be passed to the baby.
- A positive test result does not guarantee the bacteria will become active but helps assess the baby's risk.
- It is advisable for individuals in high-risk categories to take the test. High-risk categories include those in close contact with individuals infected with TB, healthcare workers, individuals with compromised immune systems, and those who have traveled to TB-prone regions.
- The test can help identify latent TB, where exposure has occurred without symptoms, which carries a high risk of transmission to the baby or developing into active TB.
- Early detection through the Mantoux test allows for timely treatment before significant damage occurs to the mother or baby.
- If already undergoing treatment for latent TB, the Mantoux test can help assess treatment effectiveness.
Potential Limitations of the TB Skin Test:
- False-positive results can occur if you have received the BCG vaccine, as your body may react to the PPD.
- False-negative results are possible, especially in individuals with a weak immune system, where the body may not react appropriately to the PPD, resulting in a bump size too small to be considered positive.
- The test cannot determine how long someone has been infected with TB.
- A positive result does not mean the person has contagious (active) TB.
A boosted reaction can occur in previously infected older adults whose sensitivity to tuberculin has decreased, or in persons of any age vaccinated with BCG or infected with mycobacteria other than M. tuberculosis complex. Two-step testing is a strategy used to reduce the likelihood of misinterpreting a boosted reaction as a recent infection, especially for individuals who will be retested periodically.
COVID-19 vaccination should not be delayed due to TB testing. TB skin tests are not expected to affect the safety or effectiveness of COVID-19 vaccines and can be performed before, during, or after a COVID-19 vaccination visit.
Incorrect administration of the PPD dose (more or less than 0.1 ml) or an injection that is too deep, preventing the formation of a wheal, invalidates the TB skin test. The skin test reaction should be read between 48 and 72 hours after administration by a trained health care worker. If a patient does not return within 72 hours, they will need to be rescheduled for another skin test. There is no risk associated with repeated TB skin test placements unless a previous test resulted in a severe reaction.
Redness alone at the skin test site usually indicates no TB infection. A firm red bump may mean TB bacteria infection. The size of the firm bump (not the red area) is measured 2 to 3 days after the test. If you are at higher risk for TB, a smaller bump may be considered a sign of infection.
Some individuals may have a positive TB skin test result even without being infected with TB bacteria, due to infection with nontuberculosis mycobacteria. Conversely, some individuals infected with TB bacteria may have a negative TB skin test result. Life-threatening illnesses like protein-calorie malnutrition, advanced cancer, and TB disease itself (notably miliary TB and TB meningitis) are associated with false-negative TB skin test results.

The TB Blood Test
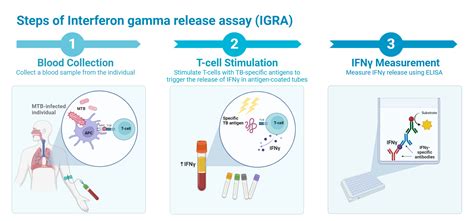
TB blood tests, also known as interferon-gamma release assays (IGRAs), use a blood sample to detect TB infection. While the TB blood test is safe to use during pregnancy, it has not been fully evaluated for diagnosing TB infection in pregnant women. However, CDC guidelines recommend using TB blood tests to test for TB infection in most cases, although TB skin tests are still recommended for children younger than 5 years of age.
BCG vaccination does not induce positive results when TB blood tests are used, making them a potentially more reliable option for individuals who have received the BCG vaccine.
TB Disease Management During Pregnancy
Pregnant women diagnosed with active TB disease can take medicine to treat the disease. Babies born to women with untreated active TB disease may have a lower birth weight than babies born to women without active TB disease. In rare cases, a baby may be born with TB.
Treatment for Latent TB Infection (LTBI) During Pregnancy
Most pregnant women can delay treatment for latent TB infection until two to three months postpartum. It may be reasonable to delay treatment until after delivery to avoid the risk of liver toxicity, an adverse effect of treatment for latent TB infection that is higher during pregnancy. However, pregnant women at higher risk for developing TB disease should not delay treatment, even during the first trimester.
There are several treatment regimens recommended for latent TB infection during pregnancy. Pregnant women taking isoniazid should also take 25-50 mg/day of pyridoxine (vitamin B6) to reduce possible adverse effects of isoniazid. Women taking isoniazid in the postpartum period should have blood tests checked for liver function before starting treatment.
Pregnant women or women expecting to become pregnant during treatment should not take the three-month weekly isoniazid and rifapentine (3HP) regimen.
Treatment for Active TB Disease During Pregnancy
Women diagnosed with TB disease during pregnancy should start treatment right away. Although the TB medicines used in recommended treatment regimens cross the placenta, these medications are not known to have harmful effects on the baby.
For pregnant women with TB disease and HIV, extrapulmonary, or severe TB disease, it may be more beneficial to include pyrazinamide in the treatment regimen. If pyrazinamide is excluded, a minimum of nine months of isoniazid, rifampin, and ethambutol is used for most pregnant women with drug-susceptible TB disease.
Health care providers may consult "Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents With HIV: Mycobacterium tuberculosis Infection and Disease."
There are known and unknown risks associated with medications for drug-resistant TB disease.
Your health care provider will choose TB medicines recommended for use during pregnancy and monitor you and your baby during treatment for inactive TB or active TB disease. It is important to report any problems experienced while taking medication.
Tuberculosis in Pregnancy; Causes, Symptoms, Diagnosis, Treatment and Pathology | TOG Article
Breastfeeding and TB Medications
Women taking first-line antituberculosis drugs may continue to breastfeed their newborns. The concentrations of these drugs in breast milk are generally too low to produce toxicity in the nursing newborn.
Rifampin can cause orange discoloration of body fluids, including breast milk. This discoloration is normal, harmless, and resolves after stopping rifampin. This effect is expected and harmless.
Risks of Untreated TB During Pregnancy
Untreated TB disease presents significant risks to both the pregnant woman and the fetus. Babies born to women with untreated TB disease are more likely to have a lower birth weight compared to babies born to women without TB. In some instances, a baby may be born with TB.
While dealing with a TB diagnosis during pregnancy is challenging, the risks associated with untreated TB disease are substantial. TB germs are spread through the air when a person with TB disease of the lungs or throat coughs, sneezes, laughs, or sings. Nearby individuals can inhale these germs and become infected.
People with TB disease feel sick due to the large number of active TB germs in their bodies. They typically exhibit one or more symptoms of TB disease. If TB disease is in their lungs, they may also experience chest pain and cough up blood.
If a pregnant woman has a positive TB test result or symptoms of TB disease, she should be evaluated for TB disease. If latent TB infection is diagnosed, short and convenient treatment regimens are available.
