Onychomycosis, commonly known as toenail fungus, is a prevalent yet challenging fungal infection affecting the nail bed, matrix, or plate. Toenails are more frequently impacted than fingernails, and this condition accounts for one-third of all integumentary fungal infections and half of all nail diseases. Onychomycosis primarily occurs in adults, with the highest incidence observed after the age of 60. While often perceived as a cosmetic issue, onychomycosis can cause significant nail disfigurement and embarrassment for those affected.
Understanding Onychomycosis
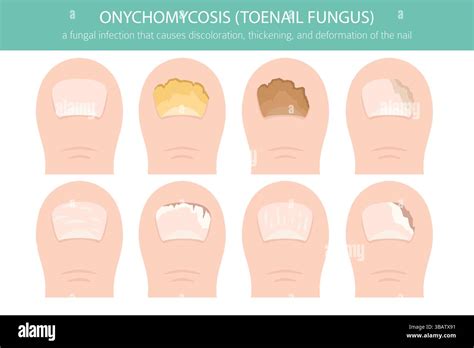
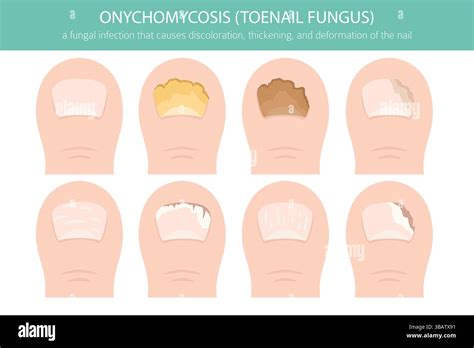
The most common form of onychomycosis is distal subungual onychomycosis, which can affect the distal and lateral aspects of the nail. This type typically begins in the toenails, fingernails, or both, and is often accompanied by some degree of tinea pedis (athlete's foot). The infection is usually caused by the fungus Trichophyton rubrum, which invades the nail bed and the underside of the nail plate, starting from the hyponychium and migrating proximally through the nail matrix.
White superficial onychomycosis constitutes about 10 percent of onychomycosis cases, predominantly affecting the toenails. In this form, fungi directly invade the superficial layers of the nail plate, creating well-defined opaque white patches that can coalesce to involve the entire nail. The affected nail becomes rough, soft, and crumbly.
Proximal subungual onychomycosis is less common in healthy individuals. It occurs when the infecting organism, typically T. rubrum, enters through the proximal nail fold, penetrates the newly formed nail plate, and then moves distally. Patients with chronic mucocutaneous candidiasis may develop candidal infections of the nails.
Total dystrophic onychomycosis can be the end result of any of the four main forms of onychomycosis.
Causes and Contagion
A type of mold known as a dermatophyte is the primary cause of tinea unguium, responsible for approximately 90% of toenail fungal infections. These microscopic organisms feed on keratin, a protein that provides hardness to nails. While dermatophytes are the most common culprits, other fungi can also infect the toenails.
Many types of toenail fungi, including tinea unguium, are highly contagious. The fungus can spread through direct contact with an infected person or by touching an infected surface. Nail fungi thrive in warm, moist, dark environments, making common areas like swimming pool perimeters, public locker rooms, and showers potential sources of infection. Walking barefoot in public areas also increases the risk.
Although toenail fungus usually remains localized to the toes, some dermatophyte fungi can spread to the skin. Onychomycosis contributes to one-third of fungal skin infections.
Symptoms of Onychomycosis
Onychomycosis can alter the appearance of the toenail in several ways:
- Color changes: Nails may turn white, yellow, or brown.
- Texture changes: Nails can appear chalky or cloudy in spots, thicken, and become misshapen.
- Nail separation: The nail may separate from the nail bed, creating a space underneath.
- Brittleness: Nails can crack or break.
While unsightly, toenail fungus is typically not painful, though some cases can become uncomfortable due to thickening and pressure on the nail bed.
Diagnosis of Onychomycosis
Accurate diagnosis is crucial, as fungi are responsible for only about half of nail dystrophies. A healthcare provider will typically examine the nails and may take clippings or scrape debris from under the nail for analysis. This is important because other conditions, such as psoriasis, and microorganisms like yeast and bacteria, can mimic fungal nail infections.
Diagnostic methods to confirm onychomycosis include:
- Potassium hydroxide (KOH) preparation: A microscopic examination of nail scrapings treated with KOH to identify fungal elements.
- Fungal culture: Growing the fungus from a nail specimen in a laboratory to identify the specific causative organism.
- Histology: Microscopic examination of a nail biopsy.
In cases of distal subungual onychomycosis, where fungal concentration is highest in the nail bed, specimens should be collected from the nail bed as close to the cuticle as possible using a curette or scalpel. For proximal superficial onychomycosis, the healthy nail plate should be gently pared away to access the infected area.
Antifungal Treatment Options
Treatment for onychomycosis depends on the severity of the infection, the number of affected nails, and the specific type of fungus causing it. It's important to note that results can take months to become apparent as the nail grows out.
Oral Antifungal Drugs
Oral antifungal medications are often the first choice for treatment due to their effectiveness. These drugs work by helping a new nail grow free of infection, gradually replacing the infected portion. Common oral agents include:
- Terbinafine (Lamisil): An allylamine antifungal agent highly effective against dermatophytes. It is typically taken daily for 6 to 12 weeks for toenail infections.
- Itraconazole (Sporanox): A triazole medication with a broad antifungal spectrum. It can be taken continuously or in an intermittent pulse-dosing regimen.
- Fluconazole (Diflucan): While not FDA-labeled for onychomycosis, early data suggest promising efficacy. Its absorption is not affected by stomach acidity.
Newer generation oral agents offer shorter treatment regimens, higher cure rates, and fewer adverse effects compared to older therapies. However, reports of terbinafine resistance are increasing globally.
Potential side effects of oral antifungal drugs can include rash and liver damage. They may also interact with other prescription medications. Regular blood tests may be required to monitor liver function during treatment.
Nail Fungus: Understanding the Infection and Nail Growth 3d Animation
Topical Treatments
Topical treatments are generally recommended for milder cases, involving less than half of the distal nail plate, or for patients who cannot tolerate systemic treatment. However, topical agents alone often struggle to penetrate the nail plate sufficiently for a complete cure.
- Medicated Nail Polish: Your healthcare provider may prescribe an antifungal nail polish, such as ciclopirox (Penlac). This is applied daily to the infected nails and surrounding skin. After seven days, the accumulated layers are wiped off with alcohol, and a new application begins.
- Medicated Nail Cream/Solution: Prescription antifungal creams like efinaconazole (Jublia) and tavaborole (Kerydin) are rubbed into the infected nails after soaking. These may be more effective if the nails are first thinned with a nonprescription lotion containing urea.
- Nonprescription Products: Several over-the-counter antifungal nail creams and ointments are available, such as terbinafine (Lamisil). For these, it is recommended to file off white markings, soak the nails, dry them thoroughly, and then apply the medicated cream or lotion.
Ciclopirox and amorolfine solutions have demonstrated some ability to penetrate all nail layers, but their efficacy as monotherapy is limited. They may be more useful as adjunctive therapy with oral treatments or for preventing recurrence.
Efinaconazole is indicated for toenail onychomycosis and has shown effectiveness against yellow streaks and dermatophytomas, which can be resistant to oral antifungals. Tavaborole is a topical oxaborole antifungal approved for onychomycosis caused by specific dermatophytes.
Combined Therapies
A combination of systemic and topical treatments can increase the cure rate. To improve outcomes and prevent recurrence, patients are often advised on proper foot hygiene, wearing breathable footwear and cotton socks, and keeping feet dry.
Nail Care and Preparation
Trimming and thinning the nails can help reduce pain by decreasing pressure. Softening thick nails with urea-containing creams before trimming or filing is also beneficial.
Alternative Medicine
Some research suggests potential benefits from certain alternative approaches:
- Biotin: This nutritional supplement may help strengthen weak or brittle fingernails.
- Tea Tree Oil: Studies indicate that tea tree oil possesses antifungal properties.
Advanced Treatment Options
For more severe or resistant cases, other therapies may be considered:
- Photodynamic Therapy (PDT) and Laser Therapy: Various laser devices, including Nd:YAG and carbon dioxide lasers, have been used. Some studies suggest laser therapy may be as effective as oral terbinafine with fewer side effects, though more extensive research is needed. Laser treatment can be combined with topical antifungals.
- Nail Avulsion: Surgical, chemical, or mechanical removal of the nail plate can be an adjunctive treatment, particularly for severe onycholysis or extensive nail thickening. Chemical nail avulsion using a urea compound is a painless option for very thick nails.

Preparing for Your Appointment
When preparing for an appointment, it's advisable to start by consulting your primary care provider or a podiatrist. Be ready to discuss any other health conditions you may have and bring any questions you have regarding brochures or printed materials.
Prognosis and Recurrence
Onychomycosis can be a persistent condition, with recurrence rates as high as 40 percent. Even with newer agents, the rate of recurrence remains high. Therefore, the decision to treat should involve a clear understanding of the associated costs, risks, and the potential for recurrence.
After antifungal therapy, disease-free nail growth should be monitored. Nails typically grow at a rate of 1.5-2 mm per month, and it may take up to a year for them to appear normal. If toenail fungus keeps returning despite preventive measures, seeking medical advice is recommended to explore underlying causes or alternative treatment approaches.
tags: #antifungal #for #onychomycosis