Changes in skin pigmentation can arise when the normal coloration of the skin is disrupted, often due to conditions like eczema. These pigmentary issues are more noticeable in individuals with darker skin tones but can occur in all skin types. The root causes are typically active eczema or the act of scratching in response to eczema-induced itch. The primary method for improving these pigmentary changes involves treating the underlying eczema and inflammation.
Understanding Pigmentation Changes in Eczema
In darker skin, inflammation can be more challenging to detect as it may manifest as various stages of hyper-pigmentation rather than visible redness. Another characteristic feature more commonly observed in darker skin is follicular prominence, where eczema appears as small, itchy bumps or papules, predominantly on the trunk and forearms.
A significant UK study on ethnic variations in atopic eczema revealed that children of African-Caribbean ethnicity were more prone to developing atopic eczema compared to their white counterparts, with a six-fold increased likelihood of severe eczema.
Causes of Darker Patches (Hyperpigmentation)
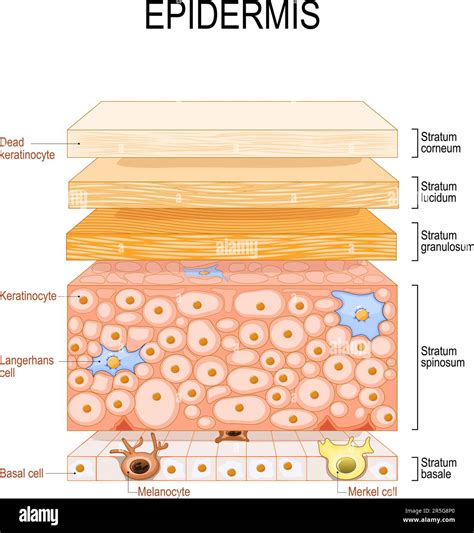
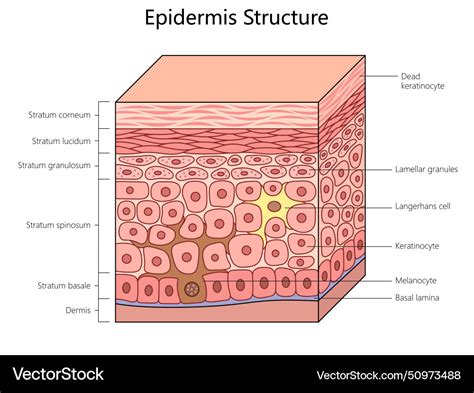
Darker patches of skin in eczema, known as hyperpigmentation, are a result of inflammation. This inflammation stimulates melanocytes, the cells responsible for skin color, to increase the production of melanin, the pigment that gives skin its color. When the skin is injured through scratching or rubbing, melanin can be released. Post-inflammatory pigmentation is another cause of darkening, occurring after eczema flare-ups have subsided. It presents as a darker patch where eczema lesions have healed. This change can be frustrating as the dark patch may persist for months, even if the eczema does not return to that area. While it affects all skin types, it is more apparent in darker skin tones.
Sunlight can exacerbate post-inflammatory pigmentation. Therefore, sun protection is crucial for all skin types to prevent its occurrence and aid in recovery.
Lichenification: Thickened Skin from Chronic Scratching
Chronic scratching and rubbing can lead to thickened areas of skin with visible scratch marks and an increase in skin markings, a condition known as lichenification. This occurs in all skin types and can manifest as a single patch, often on the dominant side of the body, such as the elbow crease or a specific body area. The scratching and rubbing can become an unconscious habit, persisting even when eczema is not actively flaring.
Hypopigmentation and Topical Treatments
Individuals with eczema sometimes worry that paler patches (hypopigmentation) are a side effect of topical treatments, particularly topical steroids. While topical steroids can temporarily dilate tiny blood vessels in the skin, this is a transient effect and not indicative of skin damage.
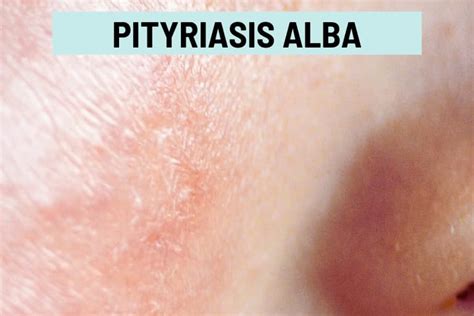
Pityriasis Alba: A Common Cause of Paler Patches
Another cause of paler patches is pityriasis alba, a mild form of eczema primarily seen in children and teenagers. It is more prevalent in darker skin than in white skin and often appears after sun exposure, as the hypo-pigmented areas do not tan, making them more conspicuous. Pityriasis alba typically presents as one to twenty round or oval patches, mainly on the face, but also on the neck, shoulders, and upper arms. Other body parts are rarely affected.
A key distinction between pityriasis alba and atopic eczema is the presence of little or no itch in pityriasis alba. However, the two conditions can coexist, in which case the eczema patches will be itchy. Patches of pityriasis alba gradually resolve, with the scaling disappearing first, followed by the restoration of normal skin tone.
Management of Pigmentary Skin Changes
While there is no specific treatment for pigmentary skin changes themselves, it is vital to recognize and treat eczema in individuals of all skin types. Over time, both hyperpigmentation and hypopigmentation will eventually resolve. It is important to remember that pigmentary changes can persist even after successful eczema treatment.
Other Conditions Causing Pigmentary Changes
Eczema is not the sole cause of pigmentary changes; various other skin conditions can contribute. Two common conditions are melasma and vitiligo.
Melasma
Hyperpigmentation on the face, and occasionally the forearms, can be attributed to melasma. This condition results from an overproduction of melanin, leading to flat, dark patches or areas of skin, most commonly on the cheeks and around the eyes. The exact cause is unknown but may be genetic and is thought to be hormonal, often seen in pregnant women or those using oral contraceptives.
Vitiligo
Vitiligo causes a loss of skin color in patches, which is usually permanent. The discolored areas typically expand over time and can affect any part of the body, including hair and the inside of the mouth.

Bowen's Disease: A Pre-cancerous Skin Condition
Bowen's disease, also known as squamous cell carcinoma in situ, is a growth of abnormal cells in the epidermis, the outermost layer of the skin. It often appears as a red, scaly area and is considered a pre-cancerous condition, with a small percentage of cases potentially progressing to squamous cell carcinoma (SCC), a common and curable form of skin cancer.
Causes and Risk Factors
Bowen's disease is most frequently linked to long-term sun exposure, with a higher risk for individuals with fair skin or those who burn easily. Occasionally, it can affect the genital area, often associated with the human papillomavirus (HPV). It can occur anywhere on the body but is typically found on sun-exposed areas.
Appearance and Diagnosis
The condition may present as raised spots or warts and can become itchy, sore, or bleed. It can be mistaken for other skin conditions like eczema or psoriasis. Diagnosis often involves a visual examination by a dermatologist, and sometimes a skin biopsy is performed for confirmation.
Treatment Options for Bowen's Disease
Treatment for Bowen's disease varies depending on the size and location of the lesion, the patient's age and health, and cosmetic concerns. Options include:
- Photodynamic Therapy (PDT): Uses a light-activated skin cream.
- Cryotherapy (Cryosurgery): Freezing the affected area, suitable for very small lesions.
- Curettage: Scraping away the affected area followed by heat or electricity to stop bleeding and destroy abnormal cells.
- Surgery: Excision of the diseased tissue.
- Laser Treatment: Uses intense light energy to remove tissue, sometimes used for lesions on fingers or genitals.
- Radiotherapy: Uses high-energy X-rays, often for symptomatic or recurrent lesions.
In some cases, if the lesion is thin and not changing, a dermatologist may advise monitoring rather than immediate treatment.
Psoriasis: A Chronic Skin Condition
Psoriasis is a chronic, hereditary skin condition affecting approximately 1.5 to 2% of the population. It is characterized by chronic, recurring scaling patches on various parts of the body. The most common form, psoriasis vulgaris, typically affects the elbows, knees, scalps, lower back, and genital areas. Other forms include guttate, inverse, pustular, and erythrodermic psoriasis.
Historical Perspective: Benjamin Franklin's Experience
Historical accounts, such as those of Benjamin Franklin, illustrate the enduring nature of psoriasis. Franklin described his ailment, which he termed "Scurf" or "Scurff," with symptoms of itching, pain, and persistent patches that align with modern descriptions of psoriasis. His writings highlight the discomfort, persistence, and psychological impact of the condition, as well as the historical search for effective treatments.
Triggers and Exacerbating Factors
Several factors can trigger or worsen psoriasis flares, including:
- Infections: Such as strep throat, thrush, viral respiratory infections, or HIV.
- Stress: Both physical (e.g., surgery) and emotional stress can significantly impact psoriasis.
- Climate: Colder climates can exacerbate psoriasis, while warmer climates, particularly those with ample sunlight, tend to improve it.
- Medications: Certain drugs can trigger or worsen psoriasis.
- Skin Injury (Koebner Phenomenon): Trauma or injury to the skin can lead to the development of psoriasis in that area.
- Lifestyle Factors: Smoking has been linked to an increased risk and severity of psoriasis, especially in women. Alcohol consumption can also exacerbate psoriasis in both men and women.
Symptoms and Associated Conditions
Psoriasis symptoms can include itching, pain, bleeding, and cracking of the skin, particularly in areas that bend. The condition can appear anywhere on the body. It is also associated with other serious health issues, including psoriatic arthritis, heart disease, and obesity.
Understanding Psoriasis
Treatment Approaches for Psoriasis
Treatment for psoriasis is individualized and may include:
- Topical Creams: Steroids, calcipotriene (a vitamin D analogue).
- Oral Medications: Methotrexate, Acitretin.
- Phototherapy: UV light therapy, including PUVA (psoralen plus UVA) and UVB.
- Biologics: Medications like Enbrel, Humira, and Remicade that target specific parts of the immune system.
Moisturizing is a crucial part of management, with recommendations for frequent application of creams and ointments. Scalp psoriasis may require specialized shampoos and topical treatments left on for an extended period.
Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN)
Stevens-Johnson syndrome (SJS) is a rare but severe disorder affecting the skin and mucous membranes, usually triggered by a reaction to medication. It begins with flu-like symptoms, followed by a painful rash that blisters and causes the top layer of affected skin to shed. Toxic epidermal necrolysis (TEN) is a more severe form of SJS.
Causes and Risk Factors
While often triggered by medications, SJS/TEN can also be caused by infections or a combination of both. Risk factors include a weakened immune system, HIV infection, cancer, and a personal or family history of SJS.
Symptoms and Complications
Symptoms include painful rash, blistering, and shedding of skin. Complications can involve eye problems (inflammation, dry eye), lung involvement, permanent skin damage, and dyspigmentation. Sepsis, a life-threatening blood infection, can also occur.
Medical Emergency and Treatment
SJS/TEN is a medical emergency requiring immediate hospitalization. Treatment focuses on removing the causative agent, wound care, pain management, and preventing complications.
Blue Skin: A Genetic Condition
The phenomenon of blue skin, as seen in the Fugate family of Kentucky, is a rare genetic condition caused by a mutation in the methemoglobinemia (met-H) gene. This mutation leads to an accumulation of methemoglobin in the blood, resulting in a bluish tint to the skin.