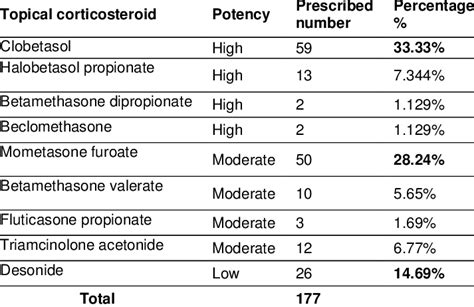
Topical corticosteroids are a cornerstone in the management of inflammatory skin conditions such as psoriasis and atopic dermatitis. These medications are categorized by their potency, which directly correlates with the potential for adverse effects. Understanding these classifications and proper application methods is crucial for safe and effective treatment.
Potency and Adverse Effects of Topical Corticosteroids
The strength of topical corticosteroids is determined by the active agent and its concentration. They are typically grouped into seven classes based on their ability to constrict blood vessels in the skin, a method assessed through the vasoconstriction assay. Many corticosteroids can fit into multiple classes depending on their concentration.
The risk of adverse effects is amplified by prolonged use, application over a large surface area, higher potency, occlusion, and use on delicate skin areas like the face and genitals. Common adverse effects include skin atrophy (thinning), striae (stretch marks), rosacea, telangiectasias (widened blood vessels), purpura (bruising), and other cutaneous and systemic reactions. Other potential cutaneous side effects encompass folliculitis, periocular dermatitis, delayed wound healing, gluteal granulomas, hypopigmentation, hypertrichosis, masking or exacerbation of fungal infections (tinea incognito), secondary infections, and contact dermatitis. Mucocutaneous infections are also frequently observed, as the anti-inflammatory action can prolong or alter the presentation of cutaneous infections. Contact sensitization to topical corticosteroids is rare.
To mitigate these risks, it is recommended to use lower-potency corticosteroids and reduce the frequency of application. For children, lower potencies and shorter treatment durations are advised. While topical corticosteroids can be used safely and effectively during pregnancy and lactation, careful consideration of risks and benefits is necessary.
Formulations and Application Methods
Topical corticosteroids are available in various formulations, each with distinct properties:
- Ointments: Petroleum-based, thick, lubricating, and occlusive. Best for dry or hyperkeratotic lesions on non-hairy skin. They leave a residue.
- Creams and Lotions: Mixtures of water and oil. Lotions have a higher water content and are more easily absorbed, vanishing into the skin. Creams are less occlusive than ointments, and lotions are less occlusive than creams. Lotions are suitable for hairy areas.
- Gels: Aqueous, dry quickly, and leave minimal residue. May sting on inflamed or eroded skin and have a drying effect.
- Foams: Easily spreadable and ideal for hairy areas like the scalp or beard.
- Solutions and Oils: Liquids that spread easily and are useful for hairy regions. Not occlusive; oils may leave a residue. Some solutions can be sprayed. Alcohol-containing solutions may sting or burn.
While ointments were traditionally considered more potent, evidence suggests that creams, lotions, and ointments have similar effectiveness. Patients often prefer creams and lotions due to their less greasy feel and easier absorption.
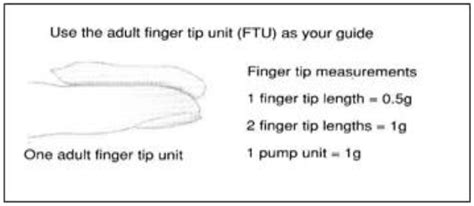
The quantity of corticosteroid prescribed is influenced by the duration of treatment, frequency of application, location on the body, and the total surface area treated. Correct patient application is paramount for successful outcomes. The fingertip unit (FTU) method is a standardized approach to measuring topical medication. One FTU is the amount dispensed from a standard 5-mm nozzle to the crease of the distal interphalangeal joint of the index finger, covering approximately 2% of an adult's body surface area.
Treatment Duration and Guidelines
The duration of treatment is dictated by the corticosteroid's strength and the condition being treated:
- Super-high-potency corticosteroids: Generally used for no more than three weeks at a time.
- High- and medium-potency corticosteroids: Typically used for up to 12 weeks.
- Low-potency corticosteroids: No specified time limit for use.
For prolonged treatment, potent corticosteroids may be used intermittently or transitioned to milder agents for maintenance. Lesions on the face, groin, and skinfolds might be treated in one- to two-week intervals. Topical corticosteroids are usually applied once or twice daily; more frequent application typically does not improve results and can decrease adherence.
Effective treatment hinges on an accurate diagnosis established through patient history, physical examination, and appropriate diagnostic tests such as biopsies or skin scrapings. Despite their widespread use, high-quality research substantiating the effectiveness of topical corticosteroids exists for a limited number of diagnoses.
Specific Considerations for Facial Use
Due to the significant risk of steroid-induced skin deterioration, potent and very potent corticosteroids are generally not recommended for use on the face, in skin folds (flexures), or on the genitalia. Mild to moderate-potency corticosteroids are the preferred treatment options for these areas.
Using strong cortisone creams or ointments on the face can lead to steroid dependence. Patients may continue using the medication due to fear of worsening their condition upon cessation, potentially exacerbating issues like acne, rosacea, perioral dermatitis, or telangiectasia. Stopping steroid use on the face after prolonged periods can result in significant rebound effects, including erythema (redness), burning, and scaling, sometimes referred to as "red face syndrome" or steroid addiction.
When treating the face, it is crucial to use only the prescribed strength and for the duration recommended by a healthcare professional. Educating patients on the appropriate amount to use and the importance of not applying to unaffected skin is vital.
Important Precautions and Potential Side Effects
Patients should be informed about potential side effects and when to seek medical attention. Along with intended effects, medications can cause unwanted reactions. These include:
Side Effects Requiring Immediate Medical Attention:
- Blistering, burning, crusting, dryness, or flaking of the skin
- Severe irritation, itching, scaling, redness, soreness, or swelling
- Redness and scaling around the mouth
- Thinning of the skin with easy bruising, especially on the face or in skin folds
- Thinning, weakness, or wasting away of the skin
- Allergic reactions (rash, itching, hives, swelling of the face, lips, or tongue)
- Burning sensation on the skin
- Dark red spots on the skin
- Infection
- Painful, red, pus-filled blisters in hair follicles
Side Effects That Usually Do Not Require Medical Attention:
- Acne or pimples
- Burning and itching of the skin with pinhead-sized red blisters
- Burning, itching, and pain in hairy areas, or pus at the root of the hair
- Increased hair growth on the forehead, back, arms, and legs
- Lightening of normal skin color
- Lightening of treated areas of dark skin
- Reddish-purple lines on the arms, face, legs, trunk, or groin
- Softening of the skin
- Dry skin, irritation
It is important to note that using too much of this medicine or using it for extended periods can increase the risk of adrenal gland problems, particularly in children. Symptoms such as blurred vision, dizziness, rapid heartbeat, increased thirst or urination, irritability, or unusual tiredness should be reported to a doctor immediately.
Patients should not use cosmetics or other skin care products on the treated areas unless advised by their doctor. If the skin condition does not improve within a few days or worsens, medical consultation is necessary.
How to use topical steroids
Patient Education and Guidance
Clear instructions for use are essential for the safe and effective application of topical corticosteroids. This includes estimating dosage in "fingertip units" and understanding the number of units required for different body parts. For instance, one unit might suffice for an adult's hand, while seven units may be needed for their back.
To prevent skin damage, corticosteroids should only be applied to affected skin areas. Enhanced education is needed to address the minimal risks associated with low to moderate strength topical corticosteroids and to emphasize the importance of using sufficient medication for effective treatment.
Treatment plans should be individualized based on the patient's symptoms, the affected body parts, and the anticipated duration of treatment. While short-term skin atrophy from treatment can often be reversed once topical corticosteroids are stopped, skin normalization may take several months.
Note: This information pertains to hydrocortisone for skin use, which is a corticosteroid. It differs from anabolic steroids. Most hydrocortisone creams and ointments are considered "mild" steroids with a lower potential for side effects compared to prescription-strength formulations.