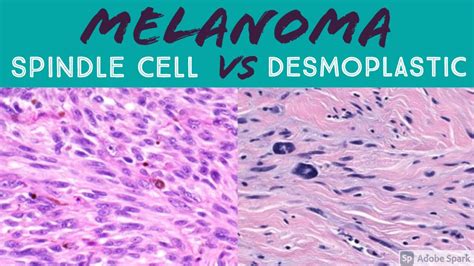
Desmoplastic melanoma and spindle cell variants of malignant melanoma are characterized by tumor cells with a spindle-shaped morphology within the dermis and/or subcutis. Desmoplastic malignant melanoma is a histologic variant of spindle cell melanoma demonstrating fibrogenic properties in which the atypical invasive malignant spindle-shaped cells are dispersed in a prominent collagenous stroma. This spindle-shaped phenotype may also demonstrate neurosustentacular properties manifesting as perineural invasion and/or Schwann cell differentiation. Spindled malignant melanocytic lesions are often described according to their predominant histologic features as spindle cell malignant melanoma, desmoplastic malignant melanoma, neurotropic/neural differentiated malignant melanoma, or any combination of these features.
Clinical Presentation
Clinically, desmoplastic malignant melanoma usually develops in the elderly on sun-exposed skin and commonly presents as a slow-growing, infiltrated, non-specific plaque or nodule that may be amelanotic in up to 50% of lesions. In the absence of clinical pigmentation, the lesion is unfortunately often mistaken for a scar or cyst. Desmoplastic melanoma is most common on sun-exposed areas of the head and neck, accounting for over 50% of cases. It presents as a slowly enlarging area of thickened skin, sometimes described as scar-like. It is often skin-colored but may be pigmented. It becomes more distinctive over time, often growing over months to years before it is recognized.
A careful clinical history is important, which includes noting previous treatments received for non-resolving lesions. Palpation is an important step, as a large majority of desmoplastic melanoma are indurated. Clinical diagnosis is aided by dermoscopy and skin biopsy (usually excision biopsy). As desmoplastic melanoma is commonly found on the head and neck, and with lentigo maligna, it is possible that if such lesions are only partially biopsied, the desmoplastic melanoma may be missed. Dermoscopy can be helpful in distinguishing desmoplastic melanoma from other skin lesions.
Histopathological Features
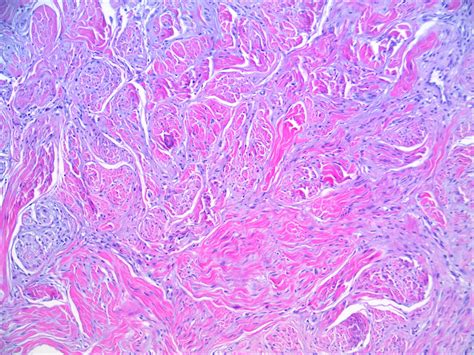
Histopathologically, desmoplastic malignant melanoma demonstrates a variably cellular spindle cell proliferation, usually non-pigmented, within a dense fibrous stroma imparting a low-power “scar-like” appearance to the lesion. The distribution of spindle cells is usually haphazard within the fibrous stroma. However, the cells may also form parallel fascicles or demonstrate a storiform pattern with associated collagen trapping mimicking a benign fibrous histiocytoma. In most cases, the proliferation is asymmetric and associated with patchy mononuclear cell inflammatory infiltrates throughout the tumor.
The cytologic atypia of the individual melanocytes varies from slight to marked and may be associated with only scant mitotic activity. Fortunately, even in cases demonstrating subtle cytologic atypia, large hyperchromatic nuclei with peripheral margination of chromatin and a prominent central magenta-colored nucleolus (typical of malignant melanoma) can often be found. In some cases, nests or fascicles of epithelioid appearing malignant melanocytes may be present and are often associated with a higher mitotic index. An overlying atypical lentiginous junctional melanocytic proliferation, representing lentigo maligna, is present in only 30% of cases. In the absence of an atypical intraepidermal component, distinguishing desmoplastic malignant melanoma with a subtle pauci-cellular proliferation of melanocytes from a scar is difficult.
At the time of diagnosis, desmoplastic melanomas are often deeply invasive with a Clark level of IV or V and an average Breslow thickness of 2.5 mm to 3.6 mm. Additional poor prognostic features include neurotropism in approximately 30% of cases.
Desmoplastic melanoma is categorized into either ‘pure’ or ‘mixed’ subtypes, which reflect the extent of desmoplasia. The Breslow thickness is reported for invasive melanomas and is measured vertically in millimeters from the top of the granular layer (or base of superficial ulceration) to the deepest point of tumor involvement. In desmoplastic melanoma, the Breslow thickness is typically thick (3-4 mm). The Clark level indicates the anatomic plane of invasion; the deeper the Clark level, the greater the risk of metastasis.
Immunohistochemistry
Spindle cell malignant melanomas are S100 positive in 94% or greater of cases. Other than in the associated epidermal component or within a second population of epithelioid appearing melanocytes, spindle cell melanoma is usually negative for Melan-A/Mart-1, HMB-45, tyrosinase, and microphthalmia transcription factor. In addition to S100, KBA.62 may prove to be another sensitive immunohistochemical marker for spindle cell melanoma. One recent study has demonstrated KBA.62 expression in 75% of desmoplastic malignant melanoma.
Neurofibroma-like desmoplastic melanoma (NFLDM) typically show SOX10 and S100 expression.
Prognosis and Behavior
Spindle cell malignant melanomas are characterized by a higher propensity for local recurrence and less frequent metastasis to regional lymph nodes at the time of presentation compared to conventional non-spindle cell melanomas. In one study of 29 patients with spindle cell melanoma (Breslow thickness 1.6 mm to 8 mm), 28 had negative sentinel lymph node biopsies. In contrast to conventional malignant melanoma, spindle cell malignant melanomas demonstrate behavior similar to soft tissue sarcoma with preferential metastasis to the lungs over regional lymph nodes. An exception to this is the presence of an epithelioid cell component within a spindle cell melanoma. These lesions, in addition to mimicking the behavior of a typical spindle cell melanoma, may demonstrate a higher rate of local regional lymph node metastasis and a worse overall prognosis compared to a malignant melanoma with a spindle-cell morphology alone.
With pure desmoplastic melanoma, the risk of regional lymph node involvement is reported to be low. Lymph nodes containing metastatic melanoma often increase in size quickly. An involved node is usually non-tender and firm to hard in consistency.
There are conflicting reports about prognostic indicators and outcomes for desmoplastic melanoma, due to its rarity, differences in pathological interpretation, and differing study designs/methodology. A study of 1129 desmoplastic melanoma patients in the United States (1992-2007) reported a 5-year specific survival rate of 85% and 10-year survival of 80%. A study of 1,735 desmoplastic melanoma patients, also in the United States (1988-2006), reported overall survival at five years to be 65% and that wide local excision was associated with increased survival.
The risk of spread and ultimate death from invasive melanoma depends on several factors, but the main one is the measured thickness of the melanoma at the time it was surgically removed. Most melanoma specialists refer to the American Joint Committee on Cancer (AJCC) cutaneous melanoma staging guidelines (8th Edition). If the local lymph nodes are enlarged due to metastatic melanoma, they should be completely removed. This requires a surgical procedure, usually under general anesthetic. If they are not enlarged, they may be tested to see if there is any microscopic spread of melanoma. In New Zealand, many surgeons recommend sentinel node biopsy for melanomas thicker than 1 mm, especially in younger persons. However, although the biopsy may help in staging cancer, it does not offer any survival advantage. Tests are not typically worthwhile for Stage 1 or Stage 2 melanoma patients unless there are signs or symptoms of disease recurrence or metastasis.
Treating Melanoma
tags: #desmoplastic #melanoma #pathology #outlines