A multidisciplinary team has uncovered a potential treatment for individuals who have suffered devastating injuries such as blast wounds and burns, which can lead to disfiguring or debilitating scars. As a wound heals, skin cells produce collagen, a protein that forms the fundamental building blocks of scar tissue. This scar tissue is inherently stiff and inflexible. When collagen production is excessive, it can result in scarring that significantly impedes natural movement or facial expressions, particularly when scars form over joints like the elbow or on the face.
"Evolutionarily, after a large injury, our bodies just want to close the wound as soon as possible to prevent infection and help control bleeding, even if it creates scar tissue," explained lead author Kellen Chen, PhD, assistant research professor in the Department of Surgery. "With modern medicine, we're trying to prevent that dysfunctional and unappealing scar tissue, and instead promote regenerative healing to have more normal skin."
Clinicians who witness the daily impact of serious wounds emphasize the need for innovations in wound care. Lourdes Castañón, MD, FACS, clinical assistant professor of surgery at the College of Medicine - Tucson and director of the Banner - University Medicine Burn Program, noted, "In severe burns, lifesaving skin grafts lead to nerve entrapment and range-of-motion-limiting contractures, which can only be addressed with lifelong surgical procedures. From a clinical care and quality of life perspective, this research is encouraging for its potential to reduce scarring and promote healthy wound healing and skin regeneration for burn victims."
Understanding the Role of FAK in Scarring
At the site of an injury, a protein known as focal adhesion kinase (FAK) initiates the production of a collagen-rich "matrix" upon which new scar tissue develops. Dr. Chen, in collaboration with Geoffrey Gurtner, MD, FACS, senior author and department chair of surgery, is investigating the efficacy of a FAK inhibitor in reducing scarring when used in conjunction with standard wound treatments. This research builds upon prior work conducted at Stanford University.
Typically, severe wounds are treated with surgically transplanted grafts of the patient's own healthy skin. These grafts are often accompanied by a hydrogel dressing, which provides wound protection and pain reduction. The Gurtner Lab observed that skin grafts treated with a hydrogel infused with the FAK inhibitor exhibited characteristics more akin to healthy skin. In contrast, untreated skin grafts produced higher levels of collagen and other "stiffer" proteins.
"Treated skin grafts are making less collagen, closer to levels found in normal, unwounded skin," stated Dr. Chen. The research team's objective is to reduce collagen production by using a FAK inhibitor, thereby enabling wounds to heal without forming excessive scar tissue, which often causes more harm than benefit.
The Microscopic Architecture of Scars
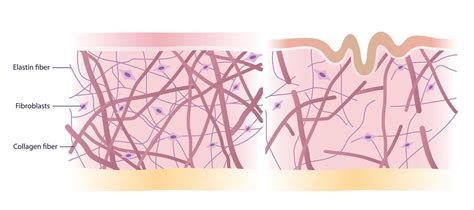
Dr. Chen elaborated that the stiffness and inflexibility of scars are not solely due to high collagen levels but also to the microscopic arrangement of collagen fibers. In healthy skin, collagen is organized in a net-like structure. However, when a wound struggles to remain closed, tensive forces cause the collagen fibers in the scar tissue to align like a bundle of ropes. This results in scar tissue that possesses strength but lacks elasticity.
"We want the healing skin to look like that net, because it has that springiness while maintaining its original strength, without being stiff," Dr. Chen explained. The Gurtner Lab's findings indicate that collagen in skin grafts treated with the FAK inhibitor was arranged more like a net than a bundle of ropes. The hope is that by treating wounds with a FAK inhibitor, scars will be smaller and more flexible, allowing for a greater range of motion in healed skin grafts and a more natural appearance.
Preparing for Human Clinical Trials
The subsequent phase involves designing a clinical trial to assess how FAK inhibitors can be incorporated into wound dressings to support the healing process in human skin grafts. Importantly, FAK inhibitors have existing clinical safety data, having been investigated in oral cancer treatments. Dr. Gurtner highlighted, "Hydrogels are commonly used in burn care, so this technology can be rapidly incorporated into the current standards of care. A topical application will be safer and easier to incorporate in the clinic because it is very similar to what we already do."
Applying the inhibitor directly to the skin allows for significantly lower doses compared to those previously tested. "We're using less than 1% of the maximum tolerated dose tested in cancer clinical trials," Dr. Chen confirmed.
Dr. Chen's foundational work involved microscopic examination of collagens to understand how physical stimuli influenced their organization. He pursued biomedical engineering with the explicit goal of patient care.
Understanding Hypertrophic Scars
What is a Hypertrophic Scar?
A hypertrophic scar is a thick, raised scar that forms as an abnormal response to wound healing, characterized by the development of extra connective tissue within the original wound area, resulting in a raised appearance.
While small wounds to the skin's top layer typically heal well, deeper wounds that penetrate the dermis trigger the body's response to repair the damage by producing collagen. Collagen is denser and less flexible than normal skin, forming scar tissue. Most scars are flat; however, excessive collagen production can lead to raised scars, classified as either hypertrophic scars or keloids.
Hypertrophic Scars vs. Keloid Scars
The primary visible distinction between hypertrophic and keloid scars lies in their spread relative to the original wound. Hypertrophic scars remain confined within the wound boundaries, whereas keloid scars extend beyond the original injury site. The following table outlines key differences:
| Feature | Hypertrophic Scars | Keloids |
|---|---|---|
| Appearance around wound | Stays within wound area | Extends beyond wound area. Can grow very large. |
| Color | Pink to red | Red to purple |
| Location on body | More common in taut skin areas | Taut and less taut skin areas |
| Collagen arrangement (microscopically) | Collagen fibers are parallel to the upper skin layer (epidermis) | Collagen fibers have random, disorganized arrangement. More blood vessels are present. |
| Time to develop | Develops 1 to 2 months after injury | Develops months to years after injury |
| Scar changing to cancer | Less frequently seen | Increased risk |
| Ease of treatment, success | Easier to treat | Harder to treat, high return rate |
| Goes away on its own | May become less noticeable with time | Never goes away without treatment |
Common Locations for Hypertrophic Scars: Hypertrophic scars are more prevalent in areas of the body with taut skin, such as the back, chest, shoulders, upper arms, and elbows, as well as other joints. However, they can appear anywhere on the skin following an injury or wound.
Risk Factors for Hypertrophic Scarring: Factors that increase the likelihood of developing hypertrophic scars include:
- Burn wounds, particularly second- and third-degree burns.
- Systemic (whole body) inflammation.
- Poor wound healing due to infection.
- Genetics: A family history of raised scarring, especially keloids, significantly increases risk.
Are Hypertrophic Scars Dangerous? No, hypertrophic scars are not dangerous or life-threatening; they primarily pose a cosmetic concern. However, they can cause pain or itching. When the body heals a wound, an overproduction of collagen can create a raised, firm scar that remains within the original injury borders. These differ from keloids, which grow beyond the wound edges and rarely shrink spontaneously. Whether recovering from surgery, a burn, or an injury, these prominent scars can be a source of concern.
A hypertrophic scar forms when the body's wound-healing process becomes overactive during the remodeling phase. Instead of producing just enough collagen to close and strengthen the wound, fibroblast cells generate excessive amounts of this structural protein. Unlike normal scars that flatten and fade over 12-18 months, hypertrophic scars can remain elevated for years without intervention. They most commonly appear after surgery, burns, deep lacerations, or other injuries affecting the deeper dermal layers of the skin.
The wound-healing timeline sheds light on why some scars become hypertrophic. During the proliferative phase, fibroblasts migrate to the wound bed and synthesize collagen to restore tissue strength. In balanced healing, collagen production and breakdown are in equilibrium. This imbalance leads to thick bundles of disorganized collagen fibers arranged in a wavy pattern, unlike the parallel basket-weave structure of normal skin. Increased blood vessel proliferation supports this active tissue, contributing to the scar's characteristic red or purple color.
Key Differences: Hypertrophic vs. Keloid vs. Normal Scars
While both hypertrophic scars and keloids stem from excessive collagen production, their behavior differs significantly. Hypertrophic scars remain within the original wound boundaries and often improve spontaneously over 1-2 years, though they rarely revert to completely normal skin. Normal scars follow a predictable pattern: they start pink or red, gradually flatten, and fade to a color close to the surrounding skin within 12-18 months. Hypertrophic scars plateau in height and color intensity but resist natural flattening. Keloids show no such plateau.
Factors Increasing Risk: Several factors heighten the likelihood of developing hypertrophic scars. Genetics play a crucial role; individuals with a family history of raised scars have a substantially increased risk. Skin pigmentation also influences scar formation, with individuals of darker skin tones (Fitzpatrick skin types IV-VI) facing a 15-20 times higher risk of both hypertrophic scars and keloids compared to lighter skin types. Anatomical location contributes as well, as scars forming over high-tension areas like the chest, shoulders, upper back, knees, ankles, and joint lines experience constant mechanical stress, stimulating ongoing collagen production. Hormonal factors are also implicated.
Prevention and Management of Hypertrophic Scars
The most effective hypertrophic scar treatment is prevention, beginning with optimal wound care from the moment of injury or surgical incision. Proper wound closure is foundational for minimizing scarring. Whether the wound is sutured, stapled, or closed with adhesive strips, the objective is to approximate skin edges with minimal tension and no gaps.
Moist Wound Healing: Maintaining a moist healing environment after closure is crucial. Contrary to the outdated advice of letting wounds "breathe," keeping wounds appropriately moist accelerates healing by 25-50% and reduces scar height. Wounds should be covered with the recommended dressing for at least 7-10 days.
Managing Mechanical Tension: Mechanical tension is a potent stimulus for hypertrophic scar development. Movement stretches the skin around a healing wound, prompting fibroblasts to produce more collagen. Steri-strips or paper tape applied perpendicular to the wound immediately after closure provide external support, offloading tension from the healing tissue. After initial healing, transitioning to silicone tape or specialized scar-prevention tapes helps maintain hydration, apply gentle pressure, and shield the scar from stretching forces.
Sun Protection: While sun exposure does not directly cause hypertrophic scars, it significantly worsens their appearance through hyperpigmentation. All healing wounds and new scars should be shielded from direct sunlight for at least one year, using a broad-spectrum SPF 30 or higher sunscreen and reapplying every two hours when outdoors. Physical blockers containing zinc oxide or titanium dioxide are particularly effective on scars due to their low potential for irritation.
Nutrition: Adequate nutrition is vital for building healthy tissue. Protein provides the amino acids necessary for collagen's basic structure, with recommendations of at least 0.8-1.0 grams per kilogram of body weight daily, increasing to 1.2-1.5 grams for large wounds or post-surgery recovery. Vitamin C is an essential cofactor for collagen synthesis, and zinc supports immune function and collagen cross-linking. Hydration is also critical, as collagen remodeling occurs in a water-rich environment.
Active Scar Management
Once a wound has closed and initial healing is complete (typically after 10-14 days), active scar management can begin at home. Silicone products are among the most studied and proven treatments for hypertrophic scar prevention and management. Multiple systematic reviews confirm that silicone gel sheets reduce scar height, redness, and stiffness with consistent use for at least 12 weeks.
- Silicone Gel Sheets: Cut the sheet slightly larger than the scar and apply it to clean, dry skin. Wear the sheet for 12-24 hours daily, removing only for cleaning. Wash the sheet daily with mild soap and water, air dry, and reapply. Sheets typically remain adhesive for 1-2 weeks before needing replacement.
- Silicone Gel Ointments: These offer an alternative for irregular surfaces, large areas, or individuals who cannot tolerate occlusive sheets. Apply a thin layer twice daily and allow it to dry, forming a flexible, breathable film.
Scar Massage: Scar massage helps reorganize collagen fibers, improve tissue flexibility, and may reduce excessive thickness by sending mechanical signals that downregulate fibroblast activity. Using fingertips or thumbs, apply firm but comfortable pressure directly to the scar. Perform linear massage by stroking across the scar perpendicular to its length, then parallel to it. This routine should be done 2-3 times daily for at least 5 minutes per session.
Pressure Garments: These provide continuous mechanical compression, reducing hypertrophic scar formation, especially on large surface areas like burns or extensive surgical sites. Pressure therapy is most effective when initiated early, ideally as soon as the wound is fully healed with no open areas, and worn consistently for 12-18 months. The garments should provide at least 15-25 mmHg pressure, fitting snugly without restricting circulation or causing pain. While pressure garments can reduce scar height by 20-30% and significantly improve softness, they do not eliminate scars entirely.
Over-the-Counter Topicals and Professional Interventions
Many over-the-counter scar treatments are available, but clinical evidence for ingredients like onion extract and vitamin E is often disappointing. Vitamin E, in particular, has failed to demonstrate benefit in controlled trials and can even cause contact dermatitis in some individuals.
For optimal results, professional intervention may be necessary for some cases. Key professional treatments include:
- Intralesional Corticosteroid Injections: Typically involving triamcinolone acetonide, these injections directly into the scar tissue reduce inflammation, suppress fibroblast activity, and promote collagen breakdown. A series of 3-6 treatments every 4-6 weeks is common. Combining triamcinolone with 5-fluorouracil (5-FU) can enhance results for scars that respond poorly to steroids alone.
- Laser Treatments: Different laser types target specific aspects of hypertrophic scar pathology. Pulsed dye laser (PDL) targets blood vessels, reducing redness. Fractional CO₂ laser creates microscopic thermal damage to the scar tissue, promoting the formation of more organized, flatter tissue. Treatment involves 3-5 sessions with significant downtime.
- Cryotherapy: Controlled freezing damages hypertrophic scar tissue, reducing height and vascularity. Surface cryotherapy applies liquid nitrogen, while intralesional cryotherapy delivers more aggressive freezing to the scar's core. Hypopigmentation is a potential risk due to melanocyte sensitivity to cold.
- Surgical Scar Revision: This involves excising the hypertrophic scar and re-closing the wound meticulously to create a thinner, less noticeable scar. It is recommended to wait at least 12-18 months after the original injury for scar maturation.
- Low-Dose Radiation Therapy: A powerful option for resistant hypertrophic scars, typically administered within 24-48 hours after surgical excision to prevent fibroblast activation. Success rates for preventing keloid recurrence after surgery can reach 80-90% with appropriate radiation.
Emerging Treatments and Lifestyle Factors
Ongoing medical research continues to advance our understanding and develop new treatment modalities:
- Microneedling (Percutaneous Collagen Induction): Creates microscopic punctures in scar tissue, triggering a wound-healing response that encourages more organized collagen.
- Botulinum Toxin (Botox): Injecting around healing wounds or scars can reduce mechanical tension by temporarily paralyzing surrounding muscles, decreasing movement and tension across the healing tissue.
- Regenerative Medicine: Research into cultured fibroblasts, adipose-derived stem cells, and bioengineered matrices aims to fundamentally alter how wounds heal, potentially preventing or reversing hypertrophic scars at a cellular level.
Scar Maturation and Documentation: Scar maturation is a lengthy process, continuing for 1 to 2 years post-injury. Monthly photo documentation using consistent lighting, distance, and angles is encouraged to track progress. Focusing on photos from three and six months prior, rather than just the previous month, provides a better perspective on long-term changes.
Stress Management: The body's stress response significantly impacts wound healing and scar remodeling. Chronic psychological stress elevates cortisol and other stress hormones that can impair collagen organization, prolong inflammation, and worsen scar formation. Adequate sleep quality is also crucial. Practical stress-management techniques include deep breathing exercises.
Clothing and Irritation: Mechanical irritation from clothing can perpetuate inflammation in remodeling scars, especially over mobile areas. Wearing soft, smooth fabrics like cotton, bamboo, or moisture-wicking athletic materials reduces friction against healing tissue.
Seeking Specialist Consultation: Patience, consistency, and a combination of preventive care and targeted interventions are key for managing hypertrophic scars. If a scar shows rapid thickening despite treatment, especially if it begins growing beyond the original wound borders, or if severe pain or itching interferes with daily life, specialist consultation is advised.
Hypertrophic Scars vs. Keloids: Hypertrophic scars do not transform into keloids; they are distinct entities. Hypertrophic scars remain within original wound boundaries and often improve with time, while keloids invade healthy tissue beyond injury margins and rarely regress spontaneously. Initial improvements in scar softness and redness are typically noticed within six to eight weeks of consistent daily use of treatments like silicone products, with significant reductions in scar height appearing after 12 to 16 weeks. Maximum benefit is usually observed after 6 to 12 months of continuous use.
Laser Treatments and Skin Tone: Laser treatments can be safe for darker skin tones when performed by experienced providers using appropriate settings and wavelengths. Pulsed dye lasers are generally effective across all skin types with adjusted parameters. Ablative lasers, such as fractional CO₂, carry a higher risk of hyperpigmentation in Fitzpatrick skin types IV through VI.
Understanding Keloid Scars
For approximately 4% to 6% of patients, the wound healing process extends too far, resulting in thick, raised scars known as keloids. These can arise from various injuries, including cuts, burns, chickenpox, acne, and piercings. Keloids can become significantly wider and taller than the original injury, growing from the size of a pencil-top eraser to much larger over months or years. Symptoms typically first appear between the ages of 10 and 30, with the 20s being a prime age for keloid development.
The impact of keloids can range from mildly annoying to socially limiting, affecting patients' quality of life similarly to psoriasis. Some individuals find it impossible to camouflage facial keloids, while others feel compelled to keep their arms and legs covered. Scarring can also cause physical issues, such as limited mobility if scars cross major joints like the shoulders, elbows, or knees. Approximately 75% of patients with keloids experience intermittent itching, and about half report scar-related pain.
What Causes Keloid Scars?
Keloids are a result of excessive collagen production by fibroblasts, a type of skin cell found in the dermis. Wounds, whether from trauma or injury, are painful and cause distress. The wound healing process is typically divided into four stages: hemostasis, inflammation, proliferation, and maturation.
- Hemostasis: The initial response to injury, involving blood vessel constriction and platelet aggregation to form a blood clot, preventing further blood loss. This phase can last up to two days.
- Inflammation: Following hemostasis, blood vessels dilate, allowing enzymes and leukocytes to enter the wound site. This stage is characterized by redness, swelling, pain, and heat and can last for six days or longer.
- Proliferation: This stage involves angiogenesis (formation of new blood vessels) and the genesis of granulation tissue-new connective tissue and blood vessels to replace damaged tissue. It depends on fibroblast synthesis and collagen production and can last over two weeks.
- Maturation (Remodeling): The final stage, which can last up to two years after the wound has sealed. Collagen builds up in the granulation tissue, forming scar tissue, and vascularity stabilizes. Cells undergo apoptosis (programmed cell death).
Excessive collagen production and cell buildup during the maturation phase result in keloid and hypertrophic scarring. This occurs when fibroblasts and keratinocytes work harder than necessary to restructure and rebuild damaged tissues. While collagen is crucial for healing, its overproduction leads to these abnormal scars.
Surgeons consider many factors when predicting scar outcomes, including the body's tendency to scar in certain areas, gentle handling of wound edges, appropriate closure techniques, and prophylactic/therapeutic strategies. Continued research is essential for preventing hypertrophic scars and keloids.
Wound Healing - Stages of healing and pathology
tags: #excessive #collagen #production #during #wound #healing