Lichenoid keratosis (LK), also known as benign lichenoid keratosis, is a common benign skin neoplasm characterized by a distinctive histological pattern. It is often referred to by several other names, including solitary lichen planus, lichen planus-like keratosis (LPLK), and involuting lichenoid plaque. This entity typically presents as a nonpruritic papule or a slightly indurated plaque on the skin.
The purpose of investigating the clinical and histopathologic features of benign lichenoid keratosis, particularly when localized on the face, is crucial for accurate diagnosis and differentiation from more serious conditions.
Clinical Presentation
Lichenoid keratosis generally develops in fair-skinned individuals, with a peak incidence between the ages of 30 and 80 years. It is observed to be twice as common in females compared to males. While often solitary, multiple eruptive lichenoid keratoses can occur, particularly on sun-exposed sites.
A study investigating benign lichenoid keratosis on the face included 14 patients diagnosed clinically and histopathologically over a 10-year period (2002-2012). Of these, 13 were female and 1 was male, with a mean age at diagnosis of 46.5 years. The majority of lesions were brown (71%), and the cheek was the most commonly affected area (71%). All lesions in this cohort were solitary. Regarding morphology, 64% of lesions were flat, and 36% were raised. While most patients denied any symptoms, three reported mild pruritus.
Clinically, LK can often be misinterpreted as other skin conditions, most notably basal cell carcinoma, due to its similar appearance. Other lesions that can mimic LK include inflamed seborrheic keratosis, Bowen's disease, inflamed lentigines, and actinic keratoses. The distinction can be challenging, making pathological evaluation essential for reliable diagnosis.
The lesion can appear as a macule or papule with a variety of colors, including pink, pinkish brown, pinkish orange, rust-colored, purplish brown, dusky violaceous, or blue-gray to black. Some lesions exhibit a velvety appearance, some have a fine scale, while others show accentuated skin markings. The size of LK can range from 3 to 20 mm in diameter, with a myriad of variations in color. Pink to red is the most common, but some may be slightly pigmented brown.
Dermoscopic Features
Dermoscopy allows for detailed visualization of structures within the epidermis, dermoepidermal junction, and papillary dermis. The dermoscopic features of lichenoid keratoses can vary depending on the stage of the lesion and the nature of the underlying growth.
In its early stage, LPLK is characterized by polymorphous vessels, including dotted vessels and short, thin vessels that can be linear, slightly curved, or serpentine. The lesions may appear structureless, pink-white with an orange or yellow hue (colors that are not bright or saturated), with scalloped borders and scale. Shiny white structures (SWS), appearing as white strands or blotches, are commonly observed.
The intermediate phase of LPLK presents with two patterns. The first pattern shows dermoscopic features of a solar lentigo (fine parallel lines, straight, slightly curved, long or short, with sharply demarcated and scalloped borders) with the addition of regression structures like focal gray dots/granules. The second pattern portrays the features of a seborrheic keratosis (sharply demarcated borders, milia-like cysts, comedo-like openings, fissures, ridges, looped vessels, and fine vessels surrounded by a halo) also with regression structures.
A recent study comparing LPLKs with non-LPLK cutaneous lesions found that LPLKs had clinical differential diagnoses including basal cell carcinoma, squamous cell carcinoma, nevus, melanoma, seborrheic keratosis, lentigo, and actinic keratosis. Dermoscopic features that distinguished LPLKs from other lesions included overall organized dermoscopic structures, scale, orange color, and coarse +/- fine granules and peppering as the only feature present. LPLKs were less likely to have moth-eaten borders and irregular dots compared to other lesions.
Dermoscopically, lichenoid keratoses are typically a reddish-brown color with a localized or diffuse brownish-grey granular pattern. Uniform clusters of grey dots are also a characteristic finding.
Histopathological Findings
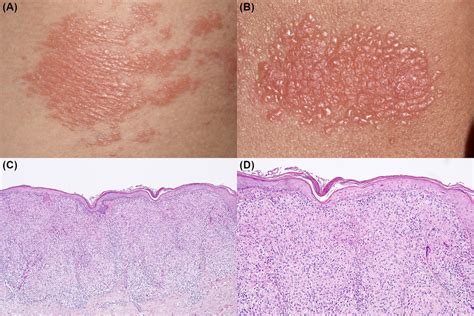
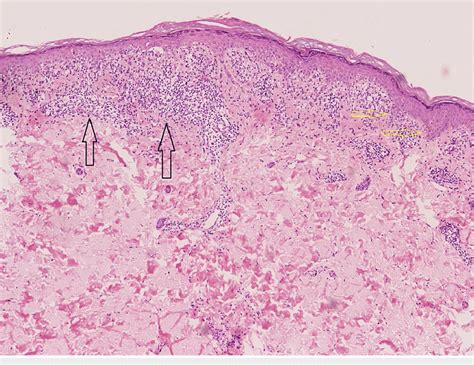
Histopathological analysis of lichenoid keratosis reveals a pronounced lichenoid inflammatory infiltrate that is nearly identical to that seen in lichen planus. This infiltrate is typically band-like and obscures the dermal-epidermal junction.
The epidermis often shows apoptotic keratinocytes (vacuolar alteration of the basal cell layer) and may exhibit epidermal acanthosis, hypergranulosis, and hyperkeratosis. Some histological features that may be present to differentiate lichenoid keratosis from lichen planus include parakeratosis and an inflammatory infiltrate containing scattered eosinophils and plasma cells. Solar elastosis and acanthosis are also frequently observed, particularly in sun-exposed skin.
In a study of 14 patients, histopathological findings indicated that all cases exhibited a lichenoid inflammatory infiltrate obscuring the dermal-epidermal junction and vacuolar alteration of the basal cell layer. The lesions frequently showed focal parakeratosis (79%), melanophages (79%), hyperkeratosis (71%), and necrotic keratinocytes (71%). Solar elastosis (50%) and acanthosis (43%) were also common. Notably, some sections showed skin with lichenoid inflammation and mild overlying hyperkeratosis with very rare parakeratosis, no significant basal atypia, and rare eosinophils. The lymphocytes did not exhibit apparent atypia.
Histology can resemble lichen planus or a lichenoid drug eruption, with some slight differences. The lesions may show focal parakeratosis, melanophages, and necrotic keratinocytes.
Differential Diagnosis and Pitfalls
Lichen planus-like keratosis is considered a great masquerader, with a differential diagnosis that includes basal cell carcinoma, squamous cell carcinoma, and melanoma. This wide differential is due to the extreme variability in characteristic appearance, with many pigmentation and morphologic possibilities.
It is important to understand that melanoma in situ with a lichenoid regression pattern may histologically mimic a lichenoid keratosis. This can occur in melanoma where a lichenoid tissue reaction may destroy or obscure nests of melanocytes in portions of the lesions. Atypical junctional melanocytic proliferations can also be seen in benign lichenoid keratosis.
Furthermore, nearly any histologically lichenoid process may simulate a lichenoid keratosis, including lichen planus, cutaneous lupus erythematosus (LE), and mycosis fungoides. In these cases, complete and accurate clinical history submitted to the pathologist is critically important.
Distinguishing LK from lichen planus can be difficult. Key histological features that may help differentiate them include a variable number of plasma cells, eosinophils, and neutrophils present in LK, as well as the presence of parakeratosis, which is typically absent in lichen planus. Clinical-pathological correlation is always necessary and is the most sensitive and specific method for differentiating these entities.
Patients with lichenoid keratoses will not exhibit mucosal lesions, nail findings, or involvement of the hair follicles, which can sometimes be seen in lichen planus. An early cutaneous lesion of lupus erythematosus may also be misinterpreted as an LK, and vice versa. Similarly, mycosis fungoides-like histological patterns have been reported in lichenoid keratosis.
A biopsy demonstrating a lichenoid appearance is key to the diagnosis. However, it is crucial to note that a biopsy might miss the diagnosis if it does not sample the entire lesion. In some instances, lichenoid keratosis can be misdiagnosed as basal cell carcinoma on biopsy due to sampling error or the presence of melanocytic lesions with lichenoid regression mimicking LK histologically.
Pathophysiology and Etiology
Lichenoid keratosis is believed to arise as an inflammatory reaction in a regressing existing solar lentigo or seborrheic keratosis. The pathophysiology is thought to be due to a chronic inflammatory-mediated involution of a pre-existing epidermal lesion, possibly a type of cell-mediated immune rejection of the overlying epidermal growth. The inciting stimulus for this inflammatory reaction remains unknown.
The epidermal growths most commonly considered precursor lesions to LK include solar lentigines and seborrheic keratoses. Reports of large cell acanthomas and viral warts have also implicated these as potential precursors.
Inflammatory Response, Animation
Management and Prognosis
The diagnosis of benign lichenoid keratosis should be made by a combination of clinical manifestations and histopathological findings. If a middle-aged patient presents with a solitary asymptomatic brown lesion on the face, benign lichenoid keratosis should be considered.
No serologic, genetic, or imaging studies are required for diagnosis; it is a clinical-pathological diagnosis. If the diagnosis is not 100% clear clinically, a biopsy is absolutely necessary.
If the biopsy confirms LK and the lesion has not been entirely removed, various destructive modalities can be employed for removal. The most straightforward method is liquid nitrogen cryotherapy. Cryotherapy followed by light curettage is another reasonable approach, as is light curettage after local anesthesia. Observation is also a completely appropriate option if the diagnosis is certain clinically and dermatoscopically.
The most common symptom associated with LK is itching, along with slight tenderness or irritation. Itching can be managed with topical corticosteroids, such as 2.5% hydrocortisone cream or triamcinolone 0.1% cream, applied twice daily. These treatments primarily help with itching and redness. Patients should be followed for the resolution of the LK over time.
If a patient begins to develop multiple lesions, the diagnosis of lichen planus should be reconsidered, especially if the areas of involvement include flexures, mucous membranes, and if there are nail findings.
There are no systemic implications associated with lichenoid keratosis. However, it is important to evaluate individuals with multiple lichenoid keratoses for the diagnosis of lichen planus. If the diagnosis is uncertain, a biopsy is crucial. If confirmed as LK, the patient can be reassured of its benign nature.