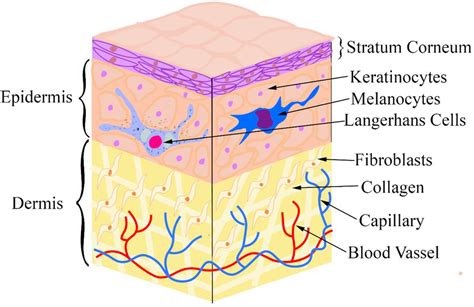
Melanoma, a term derived from "black tumor," represents the most dangerous form of skin cancer. It is characterized by rapid growth and the potential to metastasize to any organ in the body. Melanoma originates from specialized skin cells known as melanocytes, which are responsible for producing melanin, the pigment that determines skin color. While most melanomas appear black or brown, some can present as pink, red, purple, or even skin-colored lesions. Approximately 30% of melanomas develop from existing moles, while the remainder arise from normal skin. This underscores the critical importance of monitoring skin changes, as the majority of melanomas do not begin as moles. The number of moles a person has can serve as an indicator of their skin's risk for developing melanoma.
Understanding one's risk profile for melanoma is crucial. Due to the rapid progression of melanomas, delays in treatment can be life-threatening. Early detection significantly improves outcomes, with a 99% cure rate when identified in its earliest stages. The success of treatment is directly correlated with the depth of the cancerous growth.
The Incidence and Risk Factors of Melanoma
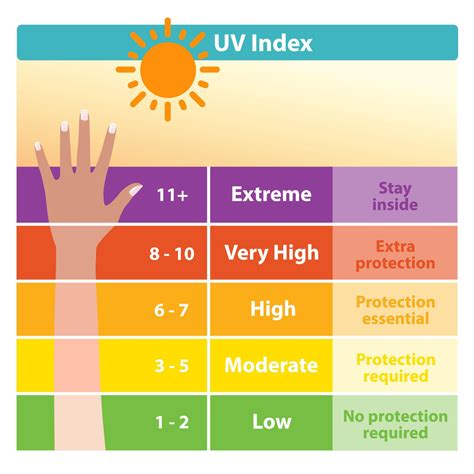
Melanoma accounts for only about 1% of all skin cancers but is responsible for the vast majority of skin cancer-related deaths. It is notably one of the most common cancers among individuals under 30, particularly young women. The incidence of melanoma has risen dramatically over the past three decades. Increasing exposure to ultraviolet (UV) radiation is widely considered a primary driver of this surge in melanoma cases.
Key Risk Factors for Melanoma:
- Family history of melanoma: A close relative with melanoma increases an individual's chances of developing the disease.
- History of sunburns: Previous severe sunburns, especially during childhood, elevate the risk.
- Exposure to UV light: Both natural sunlight and artificial sources like tanning beds and lamps are significant contributors.
- Numerous or atypical moles: Having more than 50 typical moles suggests an increased risk. Dysplastic nevi, or atypical moles, which are larger than typical moles, also heighten the risk.
- Geographic location: Living closer to the equator or at higher elevations exposes individuals to more intense UV radiation.
- Skin type: While anyone can develop melanoma, it is most common in individuals with fair skin that sunburns easily.
- Weakened immune system: Conditions or medications that suppress the immune system (e.g., post-organ transplant immunosuppressants) can increase susceptibility to melanoma and other skin cancers.
Where Melanoma Can Develop
Melanoma can manifest on any part of the body, including the eyes and internal organs. Men are more frequently diagnosed with melanoma on their trunk, often the upper back, whereas women tend to develop it more often on their legs. Melanoma can also occur in areas with minimal sun exposure, such as the soles of the feet, palms of the hands, under fingernails or toenails, and even on the scalp or genitals. These are sometimes termed "hidden melanomas."
Specific Locations and Types:
- Cutaneous Melanoma: The most common type, occurring on the skin.
- Ocular Melanoma: Melanoma within the eye, most often affecting the uvea.
- Mucosal Melanoma: Develops in the mucous membranes lining the nose, mouth, esophagus, anus, urinary tract, and vagina.
- Acral-lentiginous Melanoma: A rare form that appears under fingernails or toenails, or on the palms and soles. It is typically very dark with irregular borders.
Recognizing the Signs of Melanoma
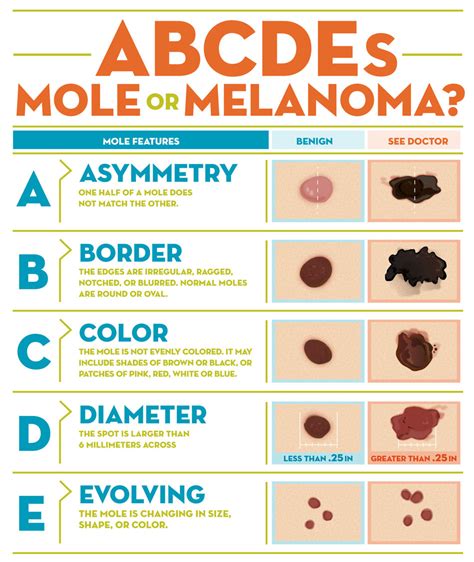
Early detection is paramount for successful treatment. Melanoma can present as moles, scaly patches, open sores, or raised bumps. The American Academy of Dermatology's "ABCDE" mnemonic is a valuable tool for identifying potential warning signs:
- Asymmetry: One half of the spot does not match the other half.
- Border: The edges are irregular, notched, or blurred.
- Color: The color is uneven, with shades of brown, black, gray, red, or white.
- Diameter: The spot is larger than the tip of a pencil eraser (approximately 6 mm).
- Evolving: The spot is new or changing in size, shape, or color.
It is important to note that some melanomas do not fit the ABCDE criteria. Any persistent sores, unusual bumps, rashes, or changes in existing moles should be brought to a doctor's attention. The "ugly duckling" sign, where a mole looks significantly different from others on the body, is also a key indicator.
Distinguishing Melanoma from Typical Moles:
Typical moles are generally uniform in color (pink, tan, brown, or black), have distinct borders, and usually appear during childhood or adolescence, with new moles potentially forming until around age 40. Adults typically have between 10 and 40 moles. Moles that are candidates for melanoma may exhibit asymmetry, color variations, changes in size or symptoms (like new itchiness or bleeding), and unusual borders.
The Development and Causes of Melanoma
Melanoma begins when healthy melanocytes undergo changes in their DNA, leading them to transform into cancer cells. DNA provides instructions for cell growth, multiplication, and death. In cancerous cells, altered DNA instructs them to multiply rapidly and survive beyond their normal lifespan, forming a tumor. These cancer cells can invade healthy tissue and spread to other parts of the body.
While the precise triggers for these DNA changes are not fully understood, a combination of environmental and genetic factors is believed to be responsible. However, healthcare professionals widely agree that exposure to ultraviolet (UV) light is the leading cause of melanoma, particularly for those cancers that develop on sun-exposed skin. UV light from the sun and tanning devices damages the DNA in skin cells.
What happens when your DNA is damaged? - Monica Menesini
Diagnosis and Staging of Melanoma
Melanoma is typically diagnosed through examinations of the skin. A biopsy, the removal of cells or tissue for microscopic examination, is essential for confirming the diagnosis. It can sometimes be challenging to differentiate between a pigmented mole and an early melanoma lesion. It is often advisable to seek a second opinion from another pathologist.
Diagnostic Procedures:
- Biopsy: Various types of skin biopsies are performed depending on the location and size of the suspicious area:
- Shave biopsy: Uses a razor blade to remove the growth.
- Punch biopsy: Employs a circular instrument to extract a core of tissue.
- Excisional biopsy: Removes the entire suspicious lesion along with a margin of normal skin.
- Sentinel Lymph Node Biopsy: Performed during surgery to check if cancer has spread to the nearest lymph nodes, which are the first to receive lymphatic drainage from the primary tumor.
- Imaging Tests: Procedures like CT scans, PET scans, and MRIs may be used to detect metastasis to other organs.
- Blood Tests: Blood chemistry studies can measure substances like lactate dehydrogenase (LDH), which may be elevated in some melanoma patients.
Staging is a critical process that describes the extent of the cancer in the body, including the tumor's size, whether it has spread to lymph nodes, and if it has metastasized to distant organs. Staging is vital for determining the most effective treatment plan.
Melanoma Staging System (TNM System):
The TNM system is commonly used, assessing:
- T (Tumor): Describes the thickness of the primary tumor and whether it is ulcerated.
- N (Nodes): Indicates whether cancer cells are present in nearby lymph nodes and their condition (e.g., matted together).
- M (Metastasis): Determines if the cancer has spread to distant parts of the body.
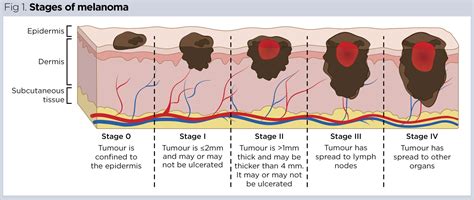
Stages of Melanoma:
- Stage 0 (Melanoma in situ): Abnormal melanocytes are confined to the epidermis (outer skin layer).
- Stage I: Early-stage melanoma, characterized by thin tumors with or without ulceration.
- Stage IA: Tumor is 1 mm thick or less, with or without ulceration.
- Stage IB: Tumor is more than 1 mm but not more than 2 mm thick, without ulceration.
- Stage II: Advanced local melanoma, with thicker tumors and/or ulceration, and potentially involvement of lymph nodes.
- Stage IIA: Tumor is 1-2 mm thick with ulceration, or 2-4 mm thick without ulceration.
- Stage IIB: Tumor is 2-4 mm thick with ulceration, or more than 4 mm thick without ulceration.
- Stage IIC: Tumor is more than 4 mm thick with ulceration.
- Stage III: Melanoma has spread to regional lymph nodes or has satellite or in-transit metastases.
- Stage IIIA: Thin tumor (â¤1 mm) with ulceration or moderate thickness (â¤2 mm) without ulceration, with cancer in 1-3 lymph nodes.
- Stage IIIB: More advanced spread to lymph nodes or skin metastases.
- Stage IIIC: Extensive spread to lymph nodes, possibly matted together, or multiple satellite/in-transit metastases.
- Stage IIID: Thick, ulcerated tumors with extensive lymph node involvement.
- Stage IV (Metastatic Melanoma): Cancer has spread to distant organs such as the lungs, liver, brain, or bone.
Treatment Options for Melanoma
Treatment for melanoma depends on the stage of the cancer, its location, and the patient's overall health. The primary goal is to remove the cancerous cells and prevent recurrence or spread.
Common Treatment Modalities:
- Wide Local Excision: Surgical removal of the melanoma along with a margin of surrounding healthy tissue to ensure all cancer cells are eliminated.
- Chemotherapy: Utilizes drugs to kill cancer cells or inhibit their division. It can be administered systemically (affecting the whole body) or regionally (targeting a specific limb).
- Immunotherapy: Harnesses the body's immune system to fight cancer.
- Targeted Therapy: Drugs that specifically target genetic mutations common in melanoma cells.
- Radiation Therapy: Uses high-energy rays to kill cancer cells, often employed for specific situations like treating brain metastases.
For patients with a history of melanoma, regular follow-up exams with a dermatologist and monthly self-exams are crucial for early detection of new primary melanomas. While the prospect of developing another melanoma can be concerning, early detection through these exams significantly increases the chances of successful treatment.
Participation in clinical trials may also be an option for individuals seeking access to new and investigational treatments. These trials play a vital role in advancing melanoma research and developing future standard treatments.