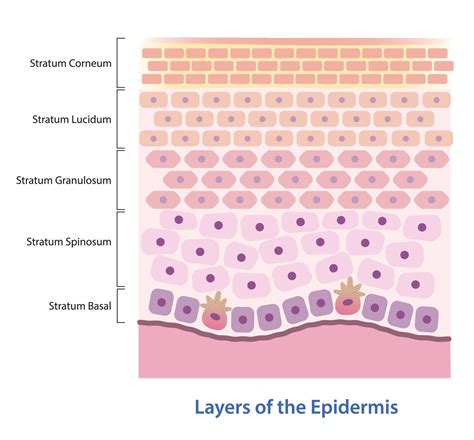
Basal cell carcinoma (BCC) is the most common type of skin cancer, accounting for the majority of skin cancer cases. It originates in the basal cells, which are found in the lowest layer of the epidermis, the outermost layer of the skin. Basal cell carcinomas can present on your skin in varying forms, including growths or lesions as red patches of skin, pink growths, open sores, and shiny bumps. Almost three million people each year are diagnosed with basal cell carcinomas. Basal cell carcinomas appear most frequently in people whose lifestyles expose them to unsafe levels of UV rays. Though the average age of basal cell carcinoma patients is declining, it is still most frequent in people over age 40. People with fair skin, blond or red hair are also more susceptible, as are people with blue, green, or grey eyes.
Basal cell carcinoma (BCC) is the most common form of skin cancer and often develops in areas of the body that are frequently exposed to the sun. Basal cell carcinoma on the face is particularly common. Other frequent sites include the neck, scalp, and arms. BCC typically presents as slow-growing lesions that rarely cause pain but may become problematic over time if untreated. These lesions may look like shiny, pearly bumps, open sores that don’t heal, or flat, scar-like areas.
Causes of Superficial Basal Cell Carcinoma
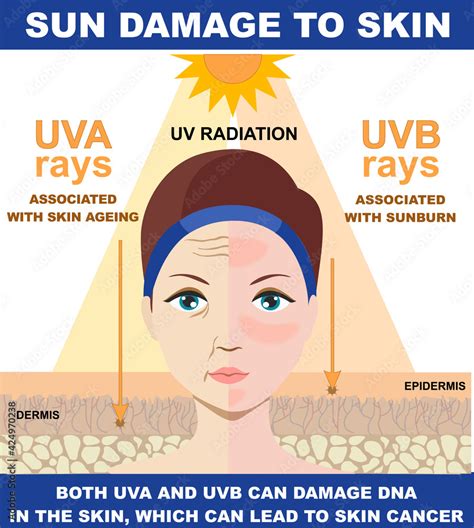
The primary cause of BCC is prolonged exposure to ultraviolet (UV) radiation from the sun or tanning beds. Basal cell carcinoma occurs when one of the skin’s basal cells develops a mutation in its DNA. A cell's DNA holds the instructions that tell the cell what to do. In healthy cells, the DNA tells the cells to grow and multiply at a set rate. The DNA also tells the cells to die at a set time.
In cancer cells, the DNA changes give different instructions. The changes tell the cancer cells to grow and multiply quickly. Cancer cells can keep living when healthy cells would die. This causes too many cells. The cancer cells can invade and destroy healthy body tissue. In time, cancer cells can break away and spread to other parts of the body. When cancer spreads, it's called metastatic cancer. Basal cell carcinoma can spread, but this is rare.
Anyone with a history of sun exposure can develop basal cell carcinoma. People who are at the highest risk have fair skin, blond or red hair, can freckle easily, and have blue, green, or grey eyes. Prolonged sun exposure or using tanning beds increases the risk of basal cell carcinoma. The threat is greater if you live in a sunny climate or a high-altitude city, both of which expose you to more UV radiation than in other locations.
Sun exposure and the use of tanning beds do not explain all the cancers that develop on the skin. For example, radiation therapy can induce DNA mutations similar to those of natural sunlight. Therefore, radiation treatments are designed to reduce risk by limiting the radiation dose or giving fewer doses. Age is also a factor. Because basal cell carcinoma often takes decades to develop, most basal cell carcinomas occur in older adults. A family history of skin cancer presents increased risk, as well as certain immune-suppressing drugs. Medications used after transplant surgery, for example, can increase risk because they suppress the immune system. Exposure to toxins, such as arsenic, can also induce similar risk.
Superficial BCC usually appears as a rough or dry pink or red patch. Ultraviolet exposure, particularly long-term exposure to sunlight (e.g., occupational exposure, working outside), is a significant factor.
Recognizing the Signs and Symptoms
Basal cell carcinoma (BCC) typically presents as slow-growing lesions that rarely cause pain but may become problematic over time if untreated. These lesions may look like:
- Shiny, pearly bumps
- Open sores that don’t heal
- Flat, scar-like areas
- Red patches of skin
- Pink growths
In some cases, BCC can appear as a dark lesion on the skin, which might look like a mole or even melanoma. Basal cell cancer on the scalp and nose is especially troublesome, with recurrences typically taking place within the first two years following surgery. Only on rare occasions do they form on unexposed areas.
Diagnosis and Examination
When seeking care for basal cell carcinoma, the whole body is examined for lesions, not just the affected area. A Total Body Skin Examination (TBSE) is a comprehensive evaluation of a person's skin from head to toe conducted by a dermatologist or healthcare professional. During this examination, the healthcare provider systematically inspects the skin, including areas that are not typically exposed to sunlight, to assess for any signs of skin cancer, abnormal moles, or other skin conditions.
A skin biopsy may be performed for suspicious moles to determine if cancer is present and which cancer it is. A diagnosis of basal cell carcinoma can only be confirmed with a biopsy. This process involves taking a small piece of the affected tissue and examining it in a laboratory. Additional tests may be needed.
Treatment Options for Superficial Basal Cell Carcinoma
Treatment for BCC depends on several factors, including the size, depth, and location of the lesion, as well as the patient’s overall health. With various effective approaches available, from surgical options to newer non-invasive therapies, it’s crucial to tailor the treatment to each case. Early intervention can improve outcomes and minimize scarring.
Surgical Treatments
Excisional Surgery
Surgical excision of the affected tissue removes the cancerous lesion and a surrounding margin of healthy skin. This helps to reduce the risk of recurrence. For small, early BCCs that have not spread, excisional surgery is frequently the only treatment required.
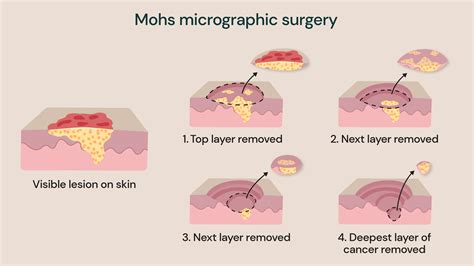
Mohs Micrographic Surgery
Yes, Mohs micrographic surgery is an effective treatment option for Basal Cell Carcinoma (BCC). Mohs surgery is a specialized and precise technique primarily used to remove skin cancers, especially those in areas where preserving healthy tissue is critical, such as the face, ears, nose, and other cosmetically sensitive regions. This precise method involves removing the cancer layer by layer while examining each layer under a microscope, ensuring minimal damage to surrounding healthy skin. Mohs surgery is often recommended for BCCs that are large, have ill-defined borders, are located in areas where tissue preservation is crucial (such as the face), or have a higher risk of recurrence. It offers high cure rates, with minimal damage to the surrounding healthy tissue, making it an excellent choice for treating certain types of Basal Cell Carcinoma. Mohs surgery is the gold standard, the most effective technique for removing BCCs, harming minimal healthy tissue while achieving the highest possible cure rate - up to 99 percent on tumors treated for the first time. It is often recommended for BCCs located in areas around the eyes, nose, lips, ears, scalp, fingers, toes, or genitals.
Curettage and Electrosurgery
Electrodesiccation and curettage involve numbing the area, scraping off the lesion with a curette (a sharp instrument with a ring-shaped tip), and then using heat or a chemical agent to destroy remaining cancer cells, control bleeding, and seal off the wound. The physician may repeat the procedure a few times during the same session until no cancer cells remain. Curettage and electrodesiccation can be effective for most small BCC lesions.
Non-Surgical Treatments
Radiation Therapy
Basal cell carcinoma radiation treatment may be recommended for older adults or those with tumors in difficult-to-operate locations. The physician uses low-energy X-ray beams to destroy the tumor, with no need for cutting or anesthesia. With radiation therapy, there is no way of knowing that all of the tumor was destroyed. Since the procedure is less precise and produces cure rates of only 90 percent, it is primarily used for BCCs that are hard to treat with surgery, and in elderly patients or people in poor health for whom surgery is not advised.
Cryotherapy
Cryotherapy is another option, which freezes the lesion with liquid nitrogen. The dermatologist uses a cotton-tipped applicator or spray device to apply liquid nitrogen to freeze and destroy the tumor. Cryosurgery is effective for smaller, superficial BCCs. It is especially useful for patients with bleeding disorders or problems tolerating anesthesia. The cure rate is between 85 and 90 percent.
Topical Therapies
Prescription creams and ointments are a viable option for small basal cell carcinomas that are less deep and when surgery is not an option. These are creams or gels applied directly to affected areas of the skin to treat superficial BCCs with minimal risk of scarring. 5-FU, a chemotherapy approved to treat certain internal cancers, has also been FDA-approved in topical form for superficial BCCs, with cure rates between 80 and 90 percent. Imiquimod is approved for superficial BCCs, with cure rates between 80 and 90 percent.
Targeted Drug Therapy and Immunotherapy
Advancements in skin cancer treatment have led to promising new therapies for basal cell carcinoma. Targeted drugs such as hedgehog pathway inhibitors are used for advanced or recurrent cases that don’t respond well to conventional treatment. Both medications are targeted drugs taken by mouth. They work by blocking the “hedgehog” signaling pathway, a key factor in the development of BCC. In 2012, vismodegib became the first medicine ever approved by the FDA for treating advanced BCC. Cemiplimab is a type of immunotherapy known as a checkpoint blockade therapy, which works by harnessing the power of the immune system to battle cancer.
Nanoparticle-based drug delivery in the fight against cancer
Prevention and Risk Reduction
While basal cell cancer is most often caused by cumulative sun exposure, many cases can be prevented or caught early with the right habits. Practicing sun protection year-round and regular skin checks can help reduce risk. The most important way to prevent BCC is to avoid sunburn. This is especially important in childhood and early life. Avoid excessive ultraviolet exposure.
Individuals with fair skin, a history of frequent sun exposure, or a family history of skin cancer are at higher risk. People over the age of 40 are also more susceptible to BCC.
Recurrence and Follow-Up
Basal cell carcinoma (BCC) can recur in the same area. About 50% of people with BCC develop a second one within 3 years of the first. They are also at increased risk of other skin cancers, especially melanoma. Therefore, regular follow-up examinations with a dermatologist are crucial, particularly for individuals with a history of BCC.
tags: #superficial #basal #skin #cancer