Chronic obstructive pulmonary disease (COPD) is a progressive lung condition characterized by lung damage that leads to airway inflammation, commonly known as swelling and irritation. This inflammation obstructs airflow into and out of the lungs. COPD is typically caused by prolonged exposure to irritants such as smoke, fumes, dust, or chemicals. The two primary forms of COPD are emphysema and chronic bronchitis. Chronic bronchitis involves inflammation of the lining of the bronchial tubes, which carry air to the lungs, leading to airflow limitations and increased mucus production. Emphysema, on the other hand, damages the tiny air sacs in the lungs called alveoli. While COPD can worsen over time, it is a treatable condition, and with appropriate management, individuals can often control symptoms and enhance their quality of life.
Symptoms of COPD often become apparent only after significant lung damage has occurred. These symptoms can include a persistent cough that may produce substantial mucus and unintentional weight loss. People with COPD frequently experience periods where their symptoms intensify beyond the typical daily variations. These episodes of worsening symptoms are termed exacerbations and can persist for several days to weeks. Triggers for exacerbations can include strong smells, cold air, air pollution, or common colds and infections.
It is advisable to consult a doctor or healthcare professional if your symptoms do not improve with treatment or if they worsen.
Causes of COPD
In developed nations, the primary cause of COPD is tobacco smoking. In developing regions, COPD often affects individuals exposed to fumes from burning fuel used for cooking and heating in homes with inadequate ventilation. While not all long-term smokers develop COPD symptoms, they may still experience lung damage that impairs lung function.
How the Lungs are Affected
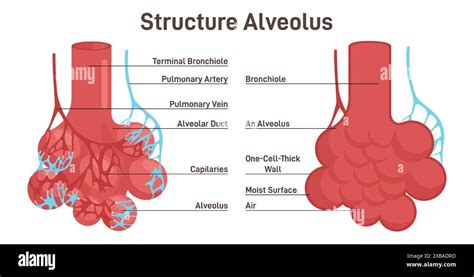
Air travels down the trachea (windpipe) into the lungs, branching into two main tubes called bronchi. Within the lungs, these tubes further divide like tree branches. The alveoli, characterized by their thin walls and rich network of tiny blood vessels, are crucial for gas exchange. Oxygen from inhaled air passes into these blood vessels and enters the bloodstream. During exhalation, the natural elasticity of the alveoli expels stale air, allowing fresh air to enter. Prolonged exposure to irritants, such as those found in cigarette smoke, damages the lungs, impeding the free movement of air. This compromised airflow limits the lungs' capacity to supply oxygen to the bloodstream and remove carbon dioxide.
Emphysema
Emphysema is a lung condition that results in the destruction of the fragile walls and elastic fibers of the alveoli. The damaged inner walls of the alveoli can break down, creating larger air spaces that are more difficult to empty compared to numerous healthy, small air sacs. This process reduces the surface area available for the exchange of oxygen and carbon dioxide.
Chronic Bronchitis
In chronic bronchitis, the bronchial tubes become inflamed and narrowed. This inflammation causes the tubes to thicken, reducing the space for air to pass through. Irritation also leads to increased mucus production, which further obstructs the narrowed tubes.
Cigarette Smoke and Other Irritants
In the majority of COPD cases in the United States, lung damage is attributed to long-term cigarette smoking. However, other factors likely contribute to COPD development, as not all smokers develop the condition.
Alpha-1-Antitrypsin Deficiency
In approximately 1% of individuals with COPD, the condition stems from a genetic mutation passed down through families, representing a hereditary form of emphysema. This genetic alteration reduces the levels of a protein called alpha-1-antitrypsin (AAT) in the body. Low AAT levels, a condition known as alpha-1-antitrypsin (AAT) deficiency, can lead to liver damage, lung conditions like COPD, or both.
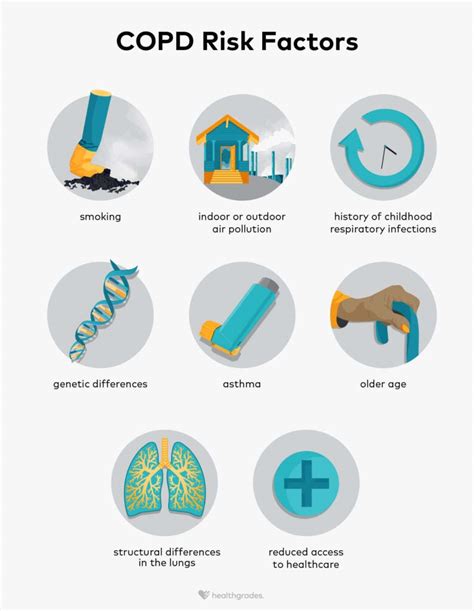
Tobacco Smoke
The most significant risk factor for COPD is long-term cigarette smoking. The duration of smoking and the number of packs consumed directly correlate with an increased risk. Smoking pipes, cigars, and marijuana may also elevate risk.
Asthma
Asthma, a condition characterized by airway narrowing, swelling, and excess mucus production, may be a risk factor for developing COPD.
Workplace Exposure
Chronic exposure to chemical fumes, smoke, vapors, and dusts in the workplace can irritate and inflame the lungs, contributing to COPD.
Fumes from Burning Fuel
Exposure to fumes from burning fuel, particularly in households with poor ventilation, is a significant cause of COPD in certain regions.
Genetics
AAT deficiency, caused by a familial gene mutation, is responsible for COPD in a subset of individuals. This genetic form of emphysema is uncommon.
Respiratory Infections
Individuals with COPD are more susceptible to infections such as colds, influenza, and pneumonia.
Complications of COPD
COPD can lead to several serious health complications, including:
- Heart problems
- Lung cancer
- High blood pressure in lung arteries: COPD can cause elevated blood pressure in the arteries that supply blood to the lungs.
- Anxiety and depression: The difficulty in breathing associated with COPD can limit engagement in enjoyable activities, potentially leading to psychological distress.
Prevention of COPD
Unlike some other medical conditions, COPD often has a clear cause and a well-defined prevention strategy. In most instances, COPD is directly linked to cigarette smoking. The most effective way to prevent COPD is to never smoke. If you have a history of smoking, quitting can be challenging, especially after multiple attempts. However, persistent effort is crucial. Engaging with a smoking cessation program can significantly increase your chances of quitting successfully and reducing further lung damage.
Workplace exposure to chemical fumes, vapors, and dusts is another preventable risk factor for COPD. If your occupation involves exposure to such lung irritants, discuss protective measures with your supervisor. Annual vaccinations against influenza and pneumococcal pneumonia are recommended to reduce the risk of respiratory infections.
COPD and Skin Rashes: Potential Connections
Individuals with COPD sometimes report experiencing itchy skin and rashes, which can negatively impact their quality of life. These skin issues may be related to the disease itself, adverse reactions to medications, or associated skin conditions.
1. Damaged Skin Barrier
Research indicates that individuals with COPD may exhibit higher skin temperatures, increased erythema (skin redness), and alterations in the skin barrier function, potentially compromising the skin's moisture retention capabilities. Studies suggest that cigarette smoke contributes to systemic inflammation, which can adversely affect skin health. A compromised skin barrier in people with COPD can manifest as itchy, irritated, dry, or thinning skin.

In cases of dry skin associated with COPD, over-the-counter moisturizers formulated for sensitive skin may offer relief. If you have a pre-existing skin condition like atopic dermatitis (eczema), diligent skin care becomes even more critical.
2. Peripheral Edema
COPD patients are at an increased risk of developing peripheral edema, which is swelling primarily in the lower legs, ankles, and feet, often due to fluid retention. This swelling can be caused by increased pressure in the lung's blood vessels, right-sided heart weakness, or reduced blood flow to the kidneys. The stretching and pressure on the skin from edema can lead to itching, discoloration, or inflammation. When blood pools in the lower legs, causing pressure on the skin, it is known as venous stasis dermatitis.
3. Shingles (Herpes Zoster)
Shingles, caused by the varicella-zoster virus, presents as an itchy and painful rash, typically on one side of the body or face, and may be accompanied by fever and chills. After a chickenpox infection, the virus remains dormant in the nervous system and can reactivate as shingles, particularly in individuals over 50. A 2011 study found that adults aged 50 and older with COPD had nearly double the risk of developing shingles compared to those without COPD.
Shingles: Pathophysiology, Symptoms, 3 stages of Infection, Complications, Management, Animation.
People living with COPD face a higher risk of developing shingles, a painful, blistering rash that often appears in a distinct stripe along one side of the body.
4. Certain Medications
Some medications used in COPD treatment can trigger allergic reactions or cause side effects like itchy skin and rashes. These may include certain corticosteroids, beta-agonists, or anticholinergic inhalers. Additionally, some painkillers, such as opioids, can induce itchy rashes as a side effect.
If you suspect a medication is causing itching or a rash, consult your doctor before making any changes to your treatment regimen, as abruptly discontinuing some medications can lead to further complications.
5. Nicotine Patches
While nicotine patches are a valuable tool for smoking cessation, they can cause skin irritation in some individuals. Typically, itching subsides within 24 hours of patch application. Persistent itching may indicate an allergic reaction, and medical advice should be sought.
Some users have reported allergic reactions to nicotine patches, characterized by severe itching and redness that lingered even after patch removal.
6. Prurigo Nodularis (PN)
Prurigo nodularis is an inflammatory skin condition linked to various medical issues, including COPD. PN causes intense itching, often preceding the appearance of a visible rash. It commonly leads to the formation of nodules (raised bumps) on the skin, which can become discolored and sore. PN can affect any area of the body prone to scratching. The itchy, firm bumps are a hallmark symptom and can vary in number and severity, appearing in various colors depending on skin tone.

The exact cause of PN is not fully understood, but it is believed to involve complex interactions within the immune system, nervous system, and skin. Diagnosing PN can be challenging due to its varied presentation. Persistent and intense itching that is difficult to pinpoint may signal PN, and a referral to a dermatologist may be necessary.
While treating PN can be complex, newer therapeutic options are showing promise for this chronic condition. Early diagnosis is key to initiating treatment and managing symptoms effectively.
When a Skin Rash May Be an Emergency
It is essential to consult your pulmonologist or dermatologist if you experience uncomfortable itching or symptoms such as hives or other skin lesions. Your healthcare team can help identify the cause of your skin issues and ensure optimal symptom management. A rash that appears suddenly and spreads rapidly could indicate a life-threatening allergic reaction or infection requiring immediate medical attention. Seek emergency care if you develop a worsening rash with blistering around the mouth, eyes, or groin, or if you have a skin infection accompanied by yellow or green discharge, swelling, or pain.