Keratosis pilaris (KP), a common and harmless skin condition, affects millions of people worldwide, manifesting as small, rough bumps often described as "chicken skin." While typically not a cause for medical concern, KP can lead to self-consciousness and a desire for smoother skin. Recent research has explored novel therapeutic approaches, including the use of non-cross-linked hyaluronic acid, showing promising results in improving the texture and appearance of the skin affected by this condition.
Understanding Keratosis Pilaris
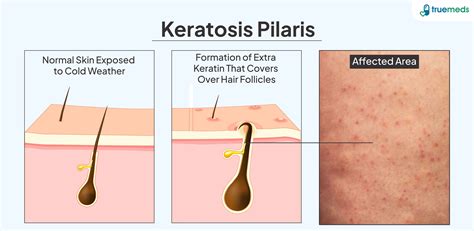
Keratosis pilaris is characterized by the buildup of keratin, a protein found in hair, skin, and nails, which forms small plugs at the openings of hair follicles. These plugs can lead to a patchwork of roughness and small bumps, sometimes accompanied by mild redness around the follicles. The condition is not contagious and is not indicative of poor hygiene. While the exact cause remains unknown, genetics are believed to play a significant role, with a family history of KP increasing the likelihood of developing it.
The bumps associated with KP are typically small, uniform, and feel rough to the touch. They are commonly found on the backs of the arms and thighs, but can also appear on the buttocks and, less frequently, on the face. While KP does not usually cause intense itching, some individuals may experience mild irritation.
It is important to distinguish KP from other skin conditions. True KP bumps are persistent and do not typically flare up dramatically and then disappear. Unlike acne, KP is not related to broken skin or infection, and aggressive scrubbing can actually worsen the appearance of the bumps by irritating the skin.
Traditional and Emerging Treatment Modalities
For many years, treatment for keratosis pilaris has focused on managing the condition rather than offering a permanent cure. Standard approaches include:
- Gentle Cleansing: Using mild, non-drying body washes to avoid further irritating the skin.
- Gentle Exfoliation: Employing ingredients that help to loosen keratin buildup, such as alpha-hydroxy acids (AHAs) like lactic acid and glycolic acid, or beta-hydroxy acids (BHAs) like salicylic acid. These are available in various over-the-counter products.
- Moisturizing: Applying thick, fragrance-free moisturizers, especially after showering, to hydrate the skin and improve its texture. Moisturizers containing humectants like hyaluronic acid can be particularly beneficial as they draw water into the skin.
- Patience: Recognizing that visible improvements can take weeks or even months of consistent care.
For more persistent cases, dermatologists may recommend prescription-strength retinoids or stronger chemical exfoliants. Advanced treatments such as microdermabrasion, chemical peels, and laser therapies (including pulsed dye and fractional CO2 lasers) can also be effective in improving skin texture and reducing redness, particularly for more inflamed presentations of KP.

The Role of Hyaluronic Acid in KP Treatment
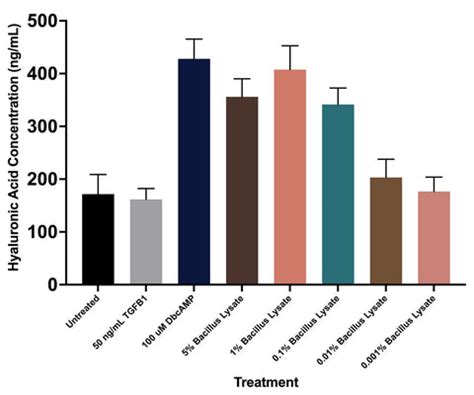
A recent study published in the Journal of Cosmetic Dermatology investigated the efficacy and safety of non-cross-linked hyaluronic acid compound dermal injections for the treatment of keratosis pilaris. This investigator-blinded, split-body, randomized, intraindividual comparative study involved 14 participants aged 18 and older diagnosed with bilateral upper extremity keratosis pilaris.
Study Design and Participants
Participants were excluded if they had received KP treatment within the past six months or used topical therapies within one month of the study's initiation. Individuals with a history of keloids, hypertrophic scarring, active skin disease, open sores, or cutaneous infections were also ineligible. Participants were randomly assigned to receive treatment on one upper extremity, with the untreated arm serving as a control. The treatment involved multiple microinjections of a non-cross-linked hyaluronic acid compound administered every four weeks.
The study sample comprised predominantly females (10 out of 14) and individuals aged 20-29 years. A diverse range of Fitzpatrick skin types (II, III, and IV) were represented. Notably, a significant proportion of participants (11 out of 14) had a family history of KP, and approximately half (6 out of 14) experienced itching related to the condition.
Key Findings and Efficacy
The study revealed significant improvements in the treated areas compared to the control arms. Physician assessments indicated a statistically significant reduction in roughness and bumpiness, with treated sides receiving a median roughness/bumpiness score of 1.0 (interquartile range 1-2) compared to 2.0 (interquartile range 2-3) for the control sides. The median total physician score, encompassing both roughness and erythema, was 3.0 for treated sides versus 4.0 for control sides, also demonstrating significant improvement.
Patient self-reports corroborated these findings, with treated sides receiving a median roughness/bumpiness score of 1.0 compared to 2.0 for the control side. Erythema scores and overall condition ratings also showed improvement on the treated sides, aligning with physician assessments.
Dermoscopic evaluations showed substantial improvements in follicular plugs and perifollicular erythema. The count of follicular plugs decreased by 73.3%, and perifollicular erythema showed a 20% reduction. While hyperpigmentation showed minimal change, histopathological examinations supported the observed improvements, with significant amelioration of hyperkeratosis and follicular plugging.
Safety and Adverse Events
The treatment was generally well-tolerated, with no unexpected adverse events reported. However, two participants (14.3%) experienced transient post-inflammatory hyperpigmentation. These findings suggest that non-cross-linked hyaluronic acid injections are a safe and effective option for managing keratosis pilaris.
Implications and Future Directions
The study authors highlighted that this research represents the first demonstration of the utility of non-crosslinked sodium hyaluronate complex in treating keratosis pilaris, proposing it as a novel therapeutic paradigm. They suggested that this approach could offer innovative insights for using hyaluronic acid in treating other dermatological conditions characterized by rough skin and hair growth abnormalities.
Further research is deemed necessary to determine the long-term efficacy of this treatment. However, the initial results are highly encouraging, suggesting a new avenue for individuals seeking to improve the appearance and texture of their skin affected by keratosis pilaris.
How Sodium Hyaluronic Acid Hydrates and Restores Skin | 3D Animation Explainer
tags: #hyaluronic #acid #keratosis #pilaris