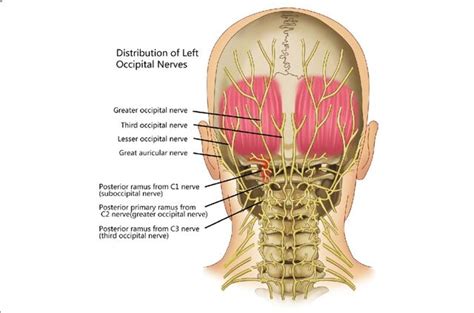
Occipital neuralgia is a neurological condition characterized by inflammation or injury to the occipital nerves. These nerves run from the top of the spinal cord at the base of the neck up through the scalp. The pain associated with occipital neuralgia can be sudden, sharp, and intense, often described as a throbbing sensation behind the eye or along the scalp. This condition can be easily confused with other headache disorders, such as migraines, due to the similarity in symptoms. However, the underlying causes and treatment approaches differ significantly, making an accurate diagnosis crucial.
What is Occipital Neuralgia?
Occipital neuralgia occurs when the occipital nerves become inflamed or injured. This irritation can lead to a range of painful sensations in the back of the head and neck. The pain typically starts at the base of the skull and can radiate upwards to the scalp, or it may be felt behind one or both eyes. Some individuals experience pain on one side of the head, while others feel it on both.
The discomfort can manifest as aching, burning, or throbbing pain. In many cases, the pain is characterized by sudden, sharp, jabbing, or electric shock-like sensations. These symptoms can be triggered by simple movements, such as combing hair, turning the head, or even lying on a pillow.
Symptoms of Occipital Neuralgia
The primary symptom of occipital neuralgia is pain, which can vary in intensity and quality. Common symptoms include:
- Aching, burning, and throbbing pain originating at the base of the head and extending to the scalp.
- Pain on one or both sides of the head.
- Pain located behind the eye.
- Sensitivity to light (photophobia), though this is more characteristic of migraines.
- Tender scalp, where even light touch can be painful.
- Pain triggered or worsened by neck movement.
- Numbness in the affected area.
- Pain behind the ears.
It's important to note that while some symptoms overlap with migraines, key distinctions exist. Migraines are typically accompanied by nausea and significant light sensitivity, which are not primary features of occipital neuralgia.
Occipital Neuralgia vs. Migraine
Distinguishing between occipital neuralgia and migraine can be challenging due to overlapping symptoms like pain at the base of the head, scalp, and behind the eyes, as well as pain with neck movement. However, migraines are often associated with nausea and heightened sensitivity to light and sound, symptoms generally absent in occipital neuralgia. Furthermore, the underlying causes differ: occipital neuralgia stems from nerve compression or irritation, while migraines are attributed to changes within the brain.

Causes of Occipital Neuralgia
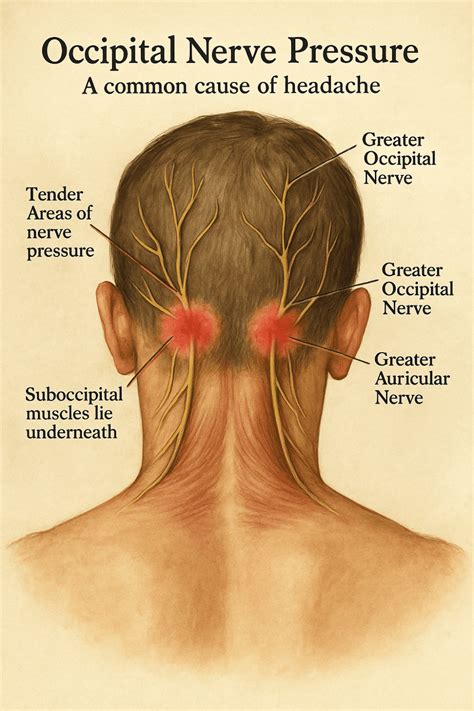
Occipital neuralgia arises from pressure or irritation to the occipital nerves. The exact cause is not always identifiable, but several factors can contribute:
- Trauma: Injury to the back of the head or neck.
- Muscle Tension: Tightness in the neck muscles can entrap and compress the occipital nerves.
- Inflammation: General inflammation in the area can affect the nerves.
- Medical Conditions: Certain conditions are linked to occipital neuralgia, including:
- Osteoarthritis
- Cervical disc disease
- Tumors in the neck
- Infections
- Gout
- Diabetes
- Blood vessel inflammation
- Pinched Nerve: A compressed nerve root in the neck, often due to arthritis.
- Prior Surgery or Injury: Scalp or skull injuries can sometimes lead to nerve irritation.
Diagnosis of Occipital Neuralgia
Diagnosing occipital neuralgia involves a comprehensive approach, as there isn't a single definitive test. A healthcare provider will typically:
- Medical History: Discuss your symptoms, their onset, duration, and any previous injuries or medical conditions.
- Physical Examination: Gently press on specific points along the occipital nerves to identify areas of tenderness and potentially reproduce the pain.
- Neurological Exam: Assess nerve function.
- Occipital Nerve Block: Injecting a local anesthetic around the occipital nerve can help confirm the diagnosis. If the injection provides significant pain relief, it strongly suggests occipital neuralgia. This can also serve as a diagnostic and therapeutic measure.
- Imaging Tests: In some cases, MRI or CT scans of the spine may be ordered to rule out other underlying causes, such as structural abnormalities or tumors.
- Ultrasound: A handheld ultrasound device may be used to visualize trigger points that could be irritating the occipital nerve.
Treatment Options for Occipital Neuralgia
The goal of treatment is to alleviate pain and manage symptoms. Options range from conservative measures to surgical interventions:
Non-Invasive and Conservative Treatments
Many individuals find relief through the following methods:
- Heat Therapy: Applying a heating pad or warm compress to the neck and scalp can soothe tight muscles and ease pain.
- Rest: Resting in a quiet, comfortable environment can help reduce sensory input and pain.
- Massage: Gentle massage of tight and painful neck muscles can release tension.
- Stretching: Specific neck stretches can help improve flexibility and reduce nerve compression.
- Over-the-Counter (OTC) Pain Relievers: Non-steroidal anti-inflammatory drugs (NSAIDs) like ibuprofen or naproxen can help reduce inflammation and pain.
Medications
If conservative treatments are insufficient, a doctor may prescribe:
- Prescription Muscle Relaxants: To alleviate muscle spasms in the neck.
- Anti-seizure Drugs: Medications such as carbamazepine (Tegretol) or gabapentin (Neurontin) can help calm overactive nerves and reduce pain signals.
- Antidepressants: Certain antidepressants, particularly tricyclic antidepressants, can be effective in managing chronic pain conditions.
- Nerve Blocks and Steroid Injections: Injections of local anesthetics and corticosteroids around the occipital nerves can provide temporary to long-term pain relief. Multiple injections over several weeks may be necessary.
- Botox Injections: Botulinum toxin injections can help reduce inflammation and nerve excitability.
Surgical Interventions
Surgery is typically considered a last resort when other treatments have failed or if there is a clear structural cause for the nerve compression.
- Microvascular Decompression: This procedure involves identifying and adjusting blood vessels that may be compressing the occipital nerve.
- Occipital Nerve Stimulation: A device called a neurostimulator is implanted to deliver electrical pulses to the occipital nerves, helping to block pain signals.
- Spinal Cord Stimulation: Electrodes are placed between the spinal cord and vertebrae to emit electrical impulses that interrupt pain signals.
- Occipital Release Surgery: An incision is made in the back of the neck to free the occipital nerve from surrounding muscles or connective tissue that may be constricting it.
- Ganglionectomy: This surgery involves removing specific nerve cells at the top of the spine.
- Intradural Cervical C1-C3 Rhizotomy: A specialized procedure targeting specific nerve roots.
F6 Occipital Nerve Stimulation Migraine Treatment; The Trial Implant
Prognosis and Outlook
Occipital neuralgia is generally not a life-threatening condition. For most individuals, treatment, including medication and conservative therapies, leads to significant pain relief. However, the pain can sometimes be chronic and may return periodically, requiring ongoing management. It is essential to consult with a healthcare professional for an accurate diagnosis and a personalized treatment plan.