The increasing interest in minimally invasive procedures has led to a demand for effective local anesthetic algorithms. The scalp, however, presents a challenge in achieving effective anesthesia due to the presence of hair shafts.
Understanding Scalp Anatomy and Anesthesia Needs
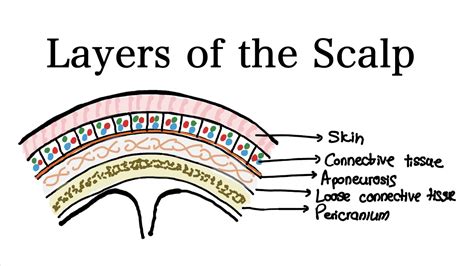
The scalp is composed of five distinct layers of soft tissue that cover the skull, extending from the supraorbital margins anteriorly to the external occipital protuberance posteriorly. These layers include a thick layer of skin containing hair and sebaceous glands, connective tissue, the epicranial aponeurosis, loose areolar tissue, and the pericranium. The skin, connective tissue, and aponeurosis are tightly bound, allowing them to slide over the underlying areolar tissue. The pericranium is a thin fascial layer attached to the outer surface of the skull, continuous with the endosteum, which explains the characteristic shape of subperiosteal hematomas.
The scalp receives blood supply from both the internal and external carotid arteries. The arterioles anastomose randomly within the connective tissue, and their containment within this rigid tissue prevents vasospasm, leading to significant bleeding in scalp lacerations.
Nerve supply to the scalp originates from the fifth cranial nerve (trigeminal) and the cervical plexus. The forehead is innervated by branches of the V1 division (supraorbital and supratrochlear nerves). The vertex and lateral scalp are supplied by V2 and V3 divisions (zygomaticotemporal, temporomandibular, and auriculotemporal nerves). The posterior scalp sensation is provided by the greater auricular and occipital nerves. These nerves become superficial and accessible for anesthetic access above an imaginary line extending from the occipital protuberance to the eyebrows, passing along the upper border of the ear. The nerves travel between the connective tissue and aponeurosis in the scalp.
Common Applications for Scalp Anesthesia
The most frequent reason for administering scalp anesthesia is the repair of lacerations or the removal of foreign bodies. While some minor lacerations may not require anesthesia, most scalp lacerations can be effectively treated with simple local infiltration. In pediatric cases, topical local anesthesia is often sufficient for laceration repair by blocking pain sensation. For larger lacerations or those requiring precise cosmetic outcomes, regional blocks of the scalp by infiltrating the major sensory nerves can be employed.
Regional scalp anesthesia is also beneficial for managing headaches of muscular and nervous origin, such as occipital headaches and trigeminal or occipital neuralgia. It serves as an excellent option for perioperative analgesia in both adults and children.
Methods of Scalp Anesthesia
Scalp anesthesia can be achieved through both subcutaneous injections and topical solutions. Subcutaneous injections can be short-acting, long-acting, or a combination, often mixed with a vasoconstricting agent like epinephrine to control bleeding. The high vascularity of the scalp generally makes the use of epinephrine safe for wound anesthesia.
Injectable Anesthetics
- Short-acting agents: Lidocaine is commonly used, available in 1% or 2% concentrations. Onset of anesthesia is typically 60-90 seconds, with effects lasting 20-30 minutes, or up to 2 hours when mixed with epinephrine.
- Long-acting agents: Bupivacaine (e.g., Sensorcaine, Marcaine) at 0.25% or 0.5% concentrations has a slower onset (10-20 minutes) but provides anesthetic effects for 4-6 hours alone, and up to 8 hours with epinephrine. Maximum doses for bupivacaine are 175 mg (2 mg/kg) in adults, increased to 225 mg (3 mg/kg) when mixed with epinephrine.
Topical Anesthetics
Preparations like LET (lidocaine 4%, epinephrine 1:1000, tetracaine 0.5%) and EMLA (lidocaine 2.5%, prilocaine 2.5%) are designed for superficial wounds and intact skin anesthesia, proving particularly advantageous for children to reduce injection discomfort. These are applied topically and covered with an occlusive dressing for about 30 minutes.
Administration Techniques
All injections should be performed under sterile conditions, with the injection site cleaned using iodine or chlorhexidine. A 25-gauge needle is recommended for minimal trauma. Shaving the skin around the wound edge is generally discouraged as it offers no proven benefit and should be avoided.
Patient positioning is important for comfort and accessibility. For forehead, vertex, or temporal regions, a supine position with the head of the bed elevated 30-45 degrees is suitable. For posterior scalp wounds or occipital headaches, a seated position or lying on the side with the head lowered is preferred.
Anesthetizing Lacerations and Abscesses
For lacerations, anesthesia is best achieved by injecting directly into the subcutaneous tissue through the wound edges, avoiding new skin punctures. For abscess drainage, anesthesia can be administered around the perimeter of the incision site via three injections in a triangular pattern, injecting into the subcutaneous tissue.
Regional Nerve Blocks
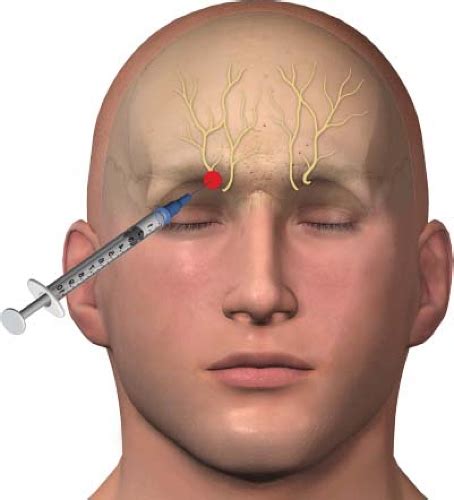
- Supraorbital Nerve Block: Anesthetizes nerves exiting the supraorbital notch. Pressure is applied to the underside of the superior orbital bone to prevent anesthetic spread into the eyelid. 1-3 mL of anesthetic is injected.
- Greater and Lesser Occipital Nerve Blocks: For the greater occipital nerve, the needle is inserted just medial to the occipital artery near the occipital protuberance and mastoid process. For the lesser occipital nerve, the needle is moved laterally and caudally from the greater occipital nerve injection site. Approximately 5 mL of anesthetic is injected for each.
Warming anesthetic medications prior to injection can reduce the burning sensation, and cooling the injection site beforehand can also improve comfort.
Scalp Numbing Sprays in Cosmetic Procedures
Tattoo numbing sprays, often containing lidocaine (e.g., 5% lidocaine), are designed to reduce pain and discomfort during tattooing. They are typically applied topically 45 minutes prior to the procedure to allow for absorption. Some formulations allow for application during the procedure.

While these sprays offer fast-acting relief that can last for several hours, it is important to be aware of potential risks. The U.S. Food and Drug Administration (FDA) has warned consumers about certain over-the-counter topical analgesic products marketed for use before, during, or after cosmetic procedures. Some products contain lidocaine at concentrations higher than permitted for over-the-counter use. When absorbed through the skin in excessive amounts, high concentrations of lidocaine can lead to serious adverse effects such as irregular heartbeat, seizures, and breathing difficulties.
The FDA advises consumers not to use such products and has issued warning letters to companies for marketing potentially dangerous products. Consumers are also advised not to wrap skin treated with these products.
Potential Complications of Scalp Anesthesia
The most common complication of scalp anesthesia is hematoma formation. Overdose, due to improper dosing, is another significant risk. Allergic reactions, infection, and failure to achieve adequate anesthesia in the target region are also potential complications.