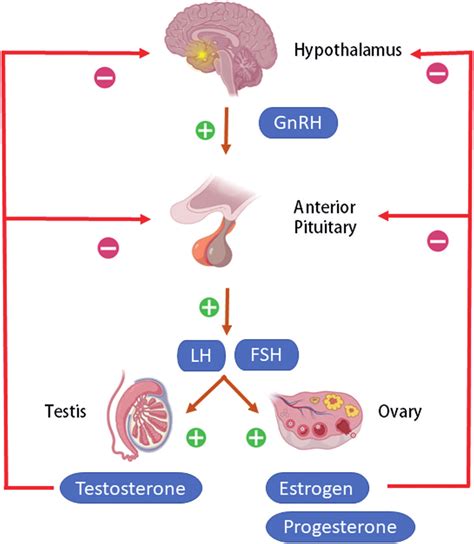
Follicle-stimulating hormone (FSH) and luteinizing hormone (LH) are critical hormones produced and released by the pituitary gland. Their synthesis and release are regulated by gonadotropin-releasing hormone (GnRH) from the hypothalamus and are further modulated by circulating gonadal steroids. Consequently, these hormones are routinely measured to assess the function of the hypothalamo-pituitary-gonadal axis.
LH and FSH play vital roles in sexual development and reproduction, influencing the function of both ovaries and testes. While FSH is named for its effect on ovarian follicles, it does not directly impact hair follicles or hair growth; androgens are responsible for hair growth.
Functions of FSH and LH
FSH Function in Fetal Development
During the second and third trimesters of pregnancy, the fetus's pituitary gland releases FSH and LH. These hormone levels peak mid-pregnancy as the first ovarian follicles or seminiferous tubules mature in the fetus.
FSH and LH Function During Puberty
FSH levels are typically low in children. As puberty approaches, the hypothalamus produces GnRH, which stimulates the pituitary gland to release FSH and LH, initiating the changes toward sexual maturity. In males, FSH and LH work together to stimulate the testes to produce testosterone, leading to physical changes like body hair growth and voice deepening, and initiating sperm production. In females, FSH and LH trigger the ovaries to produce estrogen, responsible for breast development and menstruation.
FSH Function in Menstruating Females
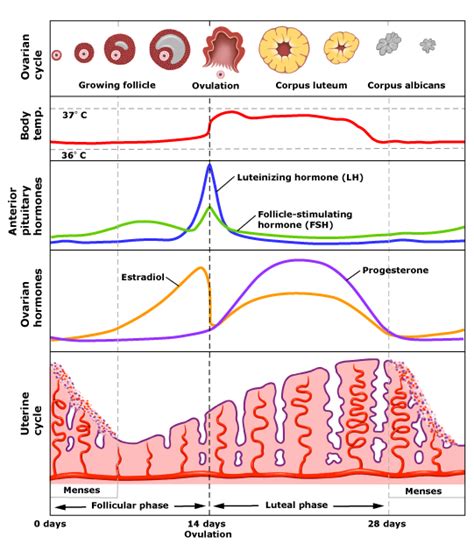
In menstruating females, FSH is crucial for regulating the menstrual cycle. It stimulates the growth of ovarian follicles, preparing eggs for ovulation. As follicles grow, they release estrogen and a small amount of progesterone. Ovulation, the release of an egg from the ovary, typically occurs around day 14 of a 28-day cycle. FSH causes follicles to mature between days six and 14, but typically only one becomes fully mature. Around day 14, an LH surge triggers the rupture of the mature follicle and egg release. After ovulation, the ruptured follicle becomes the corpus luteum, producing high levels of progesterone, which inhibits FSH release and prepares the uterine lining for potential pregnancy. If fertilization does not occur, the corpus luteum breaks down, progesterone levels decrease, and the next menstrual cycle begins with a rise in FSH.
FSH Function in Males
In males, FSH stimulates sperm production. In conjunction with testosterone, which is triggered by LH, FSH sustains this process within the testes.
Regulation of FSH Production
FSH levels are regulated by the hypothalamic-pituitary-gonadal axis. The hypothalamus releases GnRH, stimulating the pituitary to produce FSH and LH. GnRH is released in pulses; low-pulse frequencies favor FSH production, while high-pulse frequencies trigger LH production. FSH and LH then act on the testes or ovaries. Hormones released by the gonads, in turn, control GnRH release from the hypothalamus, completing the feedback loop. Estrogen in females has a complex effect: chronic exposure inhibits FSH release, while rising pre-ovulatory levels trigger increased gonadotropin release. Progesterone slows GnRH pulse frequency but enhances gonadotropin responses. In males, inhibin B from the testes blocks FSH secretion.
Indications for LH and FSH Testing
These tests are routinely used to investigate and manage:
- Fertility problems
- Menstrual irregularities (oligo/amenorrhea in younger women)
- Suspected pituitary gland disorders
- Delayed or precocious puberty
LH and FSH are not routinely recommended for diagnosing menopause in women over 45 with typical symptoms; the diagnosis is clinical. Further investigation is only warranted for atypical symptoms. FSH is not reliable in women using combined estrogen and progestogen contraception or high-dose progestogen. In women younger than 45, elevated FSH levels in two blood samples collected 4-6 weeks apart can support the diagnosis of premature menopause, provided they are not on hormonal contraception.
LH:FSH Ratios and Polycystic Ovary Syndrome (PCOS)
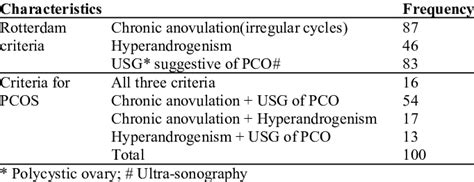
In women with PCOS, LH:FSH ratios are often raised (greater than 2.5) when samples are collected on days 1-5 of the menstrual cycle, although ratios can be normal. The diagnosis of PCOS can be made if two out of the following three criteria are met, after excluding other causes of menstrual disturbance and hyperandrogenization:
- Infrequent ovulation or anovulation (manifesting as infrequent or absent menstruation)
- Clinical or biochemical signs of hyperandrogenization (e.g., elevated testosterone and SHBG)
- Polycystic ovaries on ultrasonography
Normal FSH Levels
Normal FSH levels vary by age and sex. It's important to consult the laboratory's reference ranges for specific interpretations.
Normal FSH Levels for Males:
- Before puberty: 0 to 5.0 mIU/mL
- During puberty: 0.3 to 10.0 mIU/mL
- Adult: 1.5 to 12.4 mIU/mL
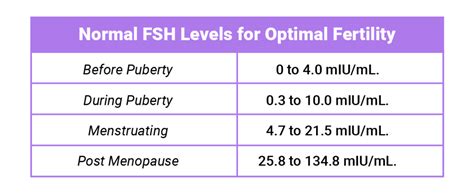
Normal FSH Levels for Females:
- Before puberty: 0 to 4.0 mIU/mL
- During puberty: 0.3 to 10.0 mIU/mL
- After puberty: 4.7 to 21.5 mIU/mL
- After menopause: 25.8 to 134.8 mIU/mL
For fertility testing, FSH is typically measured on day 3 of the menstrual cycle. Day 3 FSH levels below 15 mIU/mL are associated with a better chance of pregnancy with IVF compared to levels between 15 and 24.9 mIU/mL. Levels over 25 mIU/mL are associated with even lower pregnancy rates per attempt. However, FSH level is only one factor influencing fertility.
Conditions Associated with High FSH Levels
Elevated FSH levels often indicate an issue with the ovaries or testes (gonads). When gonads cannot produce sufficient estrogen, testosterone, or inhibin, the feedback loop is disrupted, leading to increased FSH and LH production. This is known as hypergonadotropic-hypogonadism or primary hypogonadism and is associated with primary ovarian insufficiency (POI) or testicular failure. Primary hypogonadism can be congenital (e.g., Klinefelter syndrome, Turner syndrome, androgen insensitivity syndrome) or acquired (e.g., due to gonadal toxins, injury, aging, autoimmune conditions, infections).
In females, elevated FSH levels are a normal part of menopause and perimenopause. In children, high FSH and LH levels alongside the development of secondary sexual characteristics indicate precocious (early) puberty, which is more common in females.
Conditions Associated with Low FSH Levels
Low FSH levels typically result in incomplete pubertal development and poor ovarian or testicular function in adults, leading to infertility. This condition is called hypogonadotropic-hypogonadism and is usually caused by issues with the pituitary gland or hypothalamus.
Pituitary gland issues causing low FSH include hypopituitarism, a deficiency of one or more pituitary hormones, which can be caused by pressure on the gland (e.g., from a pituitary adenoma), damage, or rare genetic conditions. Hypothalamus issues include Kallmann syndrome, an inherited condition where the hypothalamus produces insufficient GnRH, leading to low FSH and sex hormone levels and a failure to enter puberty.
Symptoms of Abnormal FSH Levels
Abnormal FSH levels, whether high or low, generally point to hypogonadism, a condition where the gonads produce insufficient sex hormones. Low FSH levels directly cause hypogonadism due to pituitary or hypothalamic dysfunction. High FSH levels are typically a consequence of hypogonadism originating in the gonads, where the pituitary gland overcompensates for the gonads' inability to produce sex hormones.
Symptoms of hypogonadism vary by age and sex:
In Newborns:
- Abnormally small penis (micropenis)
- Undescended testicles (cryptorchidism)
In Children:
- Absent breast development in females during puberty
- No or delayed menstruation
- Absent testicular enlargement in males
- Lack of a growth spurt during puberty
In Males:
- Loss of interest in sex
- Fatigue
- Infertility (likely due to low sperm count)
- Erectile dysfunction
- Breast enlargement (gynecomastia)
- Loss of muscle tone
- Reduced facial or body hair
In Females:
- Loss of interest in sex
- Fatigue
- Infertility (likely due to ovulation issues)
- Hot flashes
- Irregular or absent menstrual periods
- Loss of pubic hair
In children, high FSH and LH levels can signal precocious puberty. Low or normal FSH and LH levels in teens without signs of sexual development by age 13 (girls) or 14 (boys) usually indicate delayed puberty.

FSH Testing and Sample Requirements
FSH levels are measured through a blood test. Providers may order FSH tests along with other hormone tests, such as LH, testosterone, and estradiol, to diagnose or rule out various conditions, including infertility, ovarian or testicular dysfunction, and pituitary or hypothalamic disorders.
For women with menstrual cycles, testing is often performed on day 3. Specific sample requirements apply for patients on high-dose biotin therapy (collect at least 8 hours after the last dose). Blood is collected in specific tubes depending on age (adults, children, neonates).
Relevant clinical details are essential for interpretation, including the day of the cycle, menstrual history, fertility issues, signs of hyperandrogenization or virilization, hypogonadism, and suspected pituitary problems.
Follicle Stimulating Hormone (FSH) and Luteinizing Hormone (LH)
When to Consult a Doctor
You should contact your healthcare provider if you are experiencing symptoms of hypogonadism, if your child is entering puberty earlier or later than expected, or if you are having difficulty becoming pregnant. While many factors contribute to infertility, FSH levels can be an important indicator.