This leaflet has been written to help you understand more about squamous cell carcinoma in situ, also known as Bowen disease.
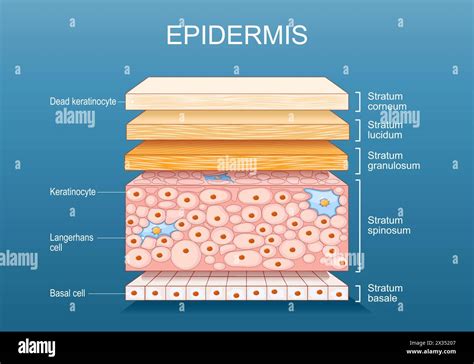
Squamous cell carcinoma in situ (SCC in situ) is a growth of cancerous cells located in the outer layer of the skin. It is often called ‘Bowen disease’ or ‘Intraepidermal carcinoma (IEC)’. SCC in situ is not a serious condition, but it can, very occasionally, progress to an invasive skin cancer known as squamous cell carcinoma (SCC).
Causes and Risk Factors
Most cases of SCC in situ develop as a result of long-term sun exposure. People who have a weakened immune system and are on long-term immunosuppression medication are more likely to get SCC in situ. Very occasionally, SCC in situ may develop after radiotherapy, longstanding arsenic ingestion (very rare nowadays) or due to the human papillomavirus (a common virus that can cause viral warts).
The most common way that your p53 gene mutates is from ultraviolet (UV) exposure from the sun, or from using indoor tanning beds. The p53 gene provides instructions for your cells to divide and replicate to replace cells when they reach the end of their lifespan. Your p53 gene is a tumor suppressor, which means that the gene controls how much and how often your cells should create new cells. Too many cells create tumors, which can be cancerous. A mutation to the p53 gene means that your cells don’t have the instructions they need to do their job correctly. As a result, your squamous cells divide and replicate too often, causing tumors (bumps, lumps or lesions) to form in and on your body.
Appearance and Location
A patch of SCC in situ starts as a small red scaly area on the skin, which grows very slowly. It may reach a diameter of a few centimetres across. It commonly occurs on skin that has been exposed to the sun, especially the face, scalp, and neck, as well as the hands and lower legs. There may be more than one area of skin affected.
A patch of squamous cell carcinoma in situ can look rather like other scaly skin conditions, such as psoriasis. For this reason, it is often examined under a dermatoscope (a magnifying tool used to examine the skin).
Bowen's disease may involve any area of the body but most frequently occurs on sun-exposed areas of the face, neck, arms, and legs. Bowen's disease occurs in sharply defined, round to irregular scaly patches. On lighter skin, the patch may look red.
The affected skin is red-brown and scaly or crusted and flat, sometimes looking like a patch of psoriasis, dermatitis, or a fungal infection called tinea or ringworm.
Diagnosis
A biopsy is the standard procedure for confirming the diagnosis of squamous cell carcinoma in situ. During this procedure, doctors remove a piece of the tumor and examine it under a microscope.
Your biopsy showed a squamous cell carcinoma in situ, meaning it is a thin skin cancer limited to the upper layers of the skin. It may grow locally but almost never spreads inside the body. It is not considered to be aggressive.
Treatment Options
If left untreated, SCC in situ will grow larger and eventually deeper into a squamous cell carcinoma. Therefore, it needs to be removed. When possible, squamous cell carcinoma in situ is usually treated with surgical removal. This can often be performed in your dermatologist’s office while you remain awake.
There are different treatment options for skin cancer. Your treatment depends on: the type of skin cancer, how far it's grown or spread, where the cancer is, and the stage of the cancer (if relevant).
Surgical Removal
Three types of surgical removal are used to treat squamous cell carcinoma in situ. The type of surgical removal you receive depends largely on the size of the tumor and where it’s located.
Excision
In an excision, the area around the skin cancer is numbed with an injection of local anesthesia. Then, a margin of normal-appearing skin around the area is cut out and the wound is closed with stitches. In all cases, the tissue removed will be sent to the pathology lab and analyzed to make sure the margins are clear and the spot has been removed. There is generally little to no wound care required at home. Stitches usually stay in between 10-14 days on the trunk and extremities, depending on the site of the surgery. Activity like vigorous exercise, tennis, or golf may be limited during that time until stitches come out. In addition, there can be no underwater submersion until the stitches have been removed. This means no swimming or baths until then. Showering after the pressure bandage has been removed, 48 hours after surgery, is fine. The recurrence rate is about 8% for skin cancer excisions. The risks of the procedure are small, but include bleeding, low risk of infection, further required surgery, cancer recurrence, and a scar.
Mohs Surgery
Mohs micrographic surgery is a specialized procedure used to treat skin cancer. It’s considered the gold standard for high-risk skin cancers, and skin cancers that appear on more delicate areas, such as the face. The procedure is indicated for circumstances when maximum tissue conservation is essential, and for cancers with hard-to-define borders. The precise nature of Mohs surgery eliminates the need to remove healthy skin. This is possible because the surgeon can remove the cancer cells in layers, and examine each under a microscope. This process is repeated until all of the cancerous cells have been removed.
Electrodessication and Curettage
In an electrodessication and curettage, or destruction, the wound is numbed with an injection of local anesthesia. This procedure is usually performed only when basal cell carcinoma develops on the trunk, an arm, or a leg. A tool called a curette is used to scrape off the cancer. An electric current in a device called a hyfrecator is used to cauterize the base. The wound heals on its own in four to twelve weeks, depending on the location. For example, it may take about four weeks to heal on the arm and three months on the lower leg, although it may be sooner. The wound heals with a circular pink to white scar. There is nothing further sent to the laboratory. The area is monitored for recurrence by the doctor. Activity under water, like in the pool or ocean, is not recommended during the extended healing time. The procedure requires daily wound care and dressings at home. The risks of the procedure are small and include bleeding, low risk of infection, scar, and recurrence of the skin cancer. The recurrence rate is about 10% for this procedure.
Non-Surgical Treatments
Other options at times include radiation therapy, which is generally not recommended as first-line therapy, or uncommonly topical therapy for specific cases of squamous cell carcinoma in situ in select cases.
- Freezing the area with liquid nitrogen (cryotherapy): This is carried out in the clinic. It can sometimes be painful, and can cause redness, puffiness, blistering or crusting, and may be slow to heal. It can be done in stages for large patches.
- Curettage: This involves scraping off the abnormal skin under a local anaesthetic.
- 5-fluorouracil cream: This is a cream that may control or completely remove SCC in situ. There are different ways of using it, and your doctor will explain to you how to best use it. It works by killing the abnormal skin cells. This means that the skin will become red and look worse during treatment, but this is temporary. After completing the course of treatment, the skin reaction should settle down over time.
- Imiquimod cream: This cream was originally developed for the treatment of genital warts but has been found useful in treating SCC in situ.
- Photodynamic therapy: A cream is applied to the skin which makes the cells in the patch of SCC in situ sensitive to particular wavelengths of light. Light from a specially designed lamp is then shone onto the patch.
- Radiotherapy and laser are other therapies occasionally used for the treatment of SCC in situ.
- Immunotherapy and chemotherapy are also mentioned as potential treatments, particularly in more advanced cases or in combination with other therapies.
Skin Cancer and Melanoma Animation
Staging and Grading
You might have tests to stage your cancer. This depends on your type of skin cancer. Most basal cell cancers (BCC) don't need staging because it's very rare for them to spread. You only need staging if your cancer is very large. You are more likely to have staging if you have squamous cell skin cancers (SCC). This is because SCCs can spread, although this is still rare.
Stage 0
Stage 0 is also called carcinoma in situ. Carcinoma means there are cancer cells. In situ means the cells are still in the place where they started to develop. So the cells have started to turn into cancer, but they have not yet spread or grown into surrounding areas of the skin. Squamous cell carcinoma in situ is also called Bowen’s disease. Bowen's disease might develop into squamous cell carcinoma (SCC) if you don't have treatment. So your doctor may describe this stage as pre-cancerous or pre-malignant.
Staging for Skin Cancer (General)
Doctors can use a numbers system or sometimes the TNM system (Tumour, Node, Metastases) to stage your cancer.
- Stage 1: The cancer is 2cm across or smaller.
- Stage 2: The cancer is larger than 2cm across, but no larger than 4cm.
- Stage 3: This can mean different things:
- Your skin cancer hasn’t spread to any lymph nodes but it: is larger than 4cm across, has grown into nearby bones causing minor damage, has grown into the space around a nerve (perineural invasion), or has grown below the layer of fat under the skin (subcutaneous tissue).
- Your cancer is smaller than 4cm but it: has spread to a single lymph node on the same side of the body as your cancer, and the lymph node is 3cm or smaller. The cancer has not spread through the outside covering of the lymph nodes.
- Stage 4: Your cancer is any size and has spread to one or more lymph nodes. And it means one or more of the following: The cancer has grown through the outside covering of one of the lymph nodes, spread to more than one lymph node, spread to only one lymph node which is larger than 3 cm and smaller than 6 cm, spread to lymph nodes on the other side of your body to the skin cancer. Or it can mean your cancer has spread to bone marrow or bone, including the bottom of the skull - and this has damaged the bone. Or your cancer has spread to another part of your body, such as the lungs (distant spread).
Staging Skin Cancer Affecting the Eyelid
Doctors use a different staging system to stage skin cancers that start in the eyelid.
- Stage 0: Carcinoma in situ.
- Stage 1: The cancer has not spread into lymph nodes or to another part of the body. It is split into 2 groups - stage 1A and 1B.
- Stage 1A: The cancer is 10mm across or smaller. It might have spread into the edge of the eyelid, or the tissue supporting the eyelid, or through the full thickness of the eyelid.
- Stage 1B: The cancer is larger than 10mm across but no larger than 20mm. It hasn’t spread into the edge of the eyelid or the tissue supporting the eyelid.
- Stage 2: The cancer has not spread into lymph nodes or to another part of the body. It is split into 2 groups - stage 2A and 2B.
- Stage 2A: Different things: the cancer is larger than 10mm across but no larger than 20mm. It has spread into the edge of the eyelid, or the tissue supporting the eyelid, or through the full thickness of the eyelid. Or the cancer is larger than 20mm across but no larger than 30mm. It might have spread into the edge of the eyelid where the eyelashes are, or the tissue supporting the eyelid, or through the full thickness of the eyelid.
- Stage 2B: The cancer is any size and has grown into nearby structures such as the eye, sinuses, tear ducts or brain.
- Stage 3: Your cancer is any size. It might have spread into the edge of the eyelid, the tissue supporting the eyelid, through the full thickness of the eyelid, or into nearby structures. It has spread to nearby lymph nodes. But it hasn’t spread to another part of your body. It is split into 2 groups - stage 3A and stage 3B.
- Stage 3A: Your cancer has spread to a single lymph node on the same side of the body as the cancer, and the lymph node is 3cm or smaller.
- Stage 3B: Different things. Your cancer has spread to: a single lymph node on the same side of the body as the cancer, and the lymph node is larger than 3cm. Or lymph nodes on the other side of the body to your eyelid cancer, or to lymph nodes on both sides of your body.
- Stage 4: Your cancer has spread to another part of your body such as your lungs.
Grades
The grade of a cancer tells you how much the cancer cells look like normal cells. The grade gives your doctor an idea of how the cancer might behave and what treatment you need. The grades of cancer cells are from 1 to 3:
- Grade 1 (low grade): look most like normal cells.
- Grade 2: look a bit like normal cells.
- Grade 3 (high grade): look very abnormal and not like normal cells.
Symptoms and Signs
Symptoms of squamous cell carcinoma include skin changes like:
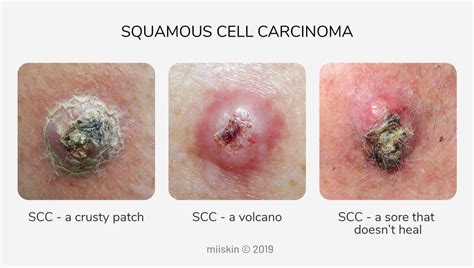
- A rough-feeling, bump or growth, which might crust over like a scab and bleed.
- A growth that’s higher than the skin around it but sinks down (depression) in the middle.
- A wound or sore that won’t heal, or a sore that heals and then comes back.
- An area of skin that’s flat, scaly and red that’s larger, about 1 inch (2.5 centimeters).
There are cancerous bumps, marks or lesions that form on your skin that can be a sign of squamous cell carcinoma, including:
- A bump or lump that can feel dry, itchy, scaly or have a different color from the skin around it (actinic keratosis).
- A lesion on your lower lip where the tissue becomes pale, dry and cracked (cheilitis). This may have a burning sensation when you’re exposed to the sun.
- White or pale spots in your mouth, on your tongue, gums or cheeks (leukoplakia).
Prevention
Because squamous cell carcinomas seem to be related to UV light exposure, doctors recommend a number of measures to limit UV light exposure, starting in early childhood:
- Avoiding the sun: For example, seeking shade, minimizing outdoor activities between 10 AM and 4 PM (when the sun’s rays are strongest), and avoiding sunbathing and the use of tanning beds.
- Wearing protective clothing: For example, long-sleeved shirts, pants, and broad-brimmed hats.
- Using sunscreen: At least sun protection factor (SPF) 30 with UVA and UVB protection used as directed and reapplied every 2 hours and after swimming or sweating but not used to prolong sun exposure.
Sun protection is recommended for all patients. Protect your skin with clothing. It is important to avoid sunburn, which is a sign of damage to your skin and increases your risk of developing a skin cancer in the future. Use a ‘high protection’ sunscreen of at least SPF 30 which also has high UVA protection.
Routine sun protection is rarely necessary in the UK for people of colour, particularly those with black or dark brown skin tones. However, there are important exceptions to this; for example, sun protection is important if you have a skin condition, such as photosensitivity, vitiligo or lupus, or if you have a high risk of skin cancer, especially if you are taking immunosuppressive treatments (including organ transplant recipients) or if you are genetically pre-disposed to skin cancer.

Prognosis and Considerations
The smaller your patch of squamous cell carcinoma in situ is, the better the results of treatment are likely to be. If the patch changes in any way, it is important to inform your doctor.
A particular problem with SCC in situ is that it frequently occurs on the lower legs. The skin on the lower legs is often tight and sometimes quite fragile, especially in older people. Healing in this area is slow.
Cutaneous squamous cell carcinoma rarely spreads to other parts of your body (metastasizes). If this does happen, it occurs slowly and can be life-threatening if left untreated.
The British Association of Dermatologists recommend that you tell your doctor about any changes to a mole or patch of skin. If your GP is concerned about your skin, you should be referred to a Consultant Dermatologist at no cost to yourself through the NHS.
The evidence relating to the health effects of serum vitamin D levels, exposure to sunlight and vitamin D intake, is inconclusive. People who are avoiding (or need to avoid) sun exposure may be at risk of vitamin D deficiency and should consider having their serum vitamin D levels checked.